

Case Reports
doi: 10.1136/bcr-2015-209732.
The difficulty in diagnosing X linked adrenoleucodystrophy and the importance of identifying cerebral involvement
Affiliations
- PMID: 25969497
- PMCID: PMC4434265
- DOI: 10.1136/bcr-2015-209732
Item in Clipboard
Case Reports
The difficulty in diagnosing X linked adrenoleucodystrophy and the importance of identifying cerebral involvement
BMJ Case Rep.
.
Abstract
Two patients are described, a mother and son, who were initially clinically diagnosed with hereditary spastic paraparesis. This was rectified after very long chain fatty acid testing confirmed adrenomyeloneuropathy (AMN). The son's initial symptoms were characteristic of AMN (the commonest phenotype) but progressed to show symptoms of cerebral involvement. This evolution from non-cerebral to cerebral AMN is recognised in the medical literature and is increasingly important to consider in light of the availability of potential treatments such as haematopoietic stem cell transplantation.
2015 BMJ Publishing Group Ltd.
Figures
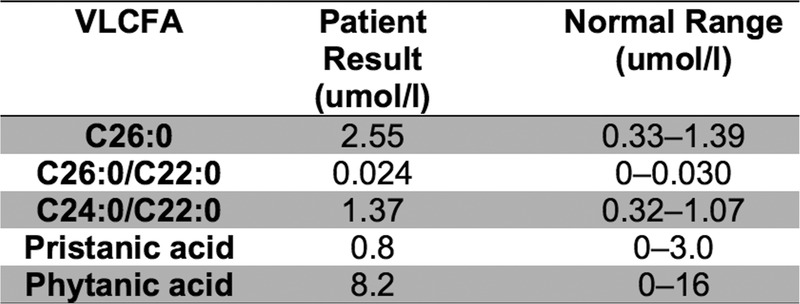
Very long chain fatty acid results for patient 1.
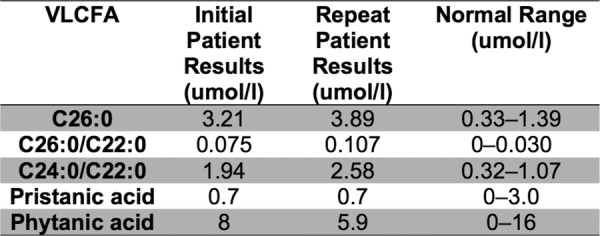
The initial and repeat very long chain fatty acid results for patient 2.
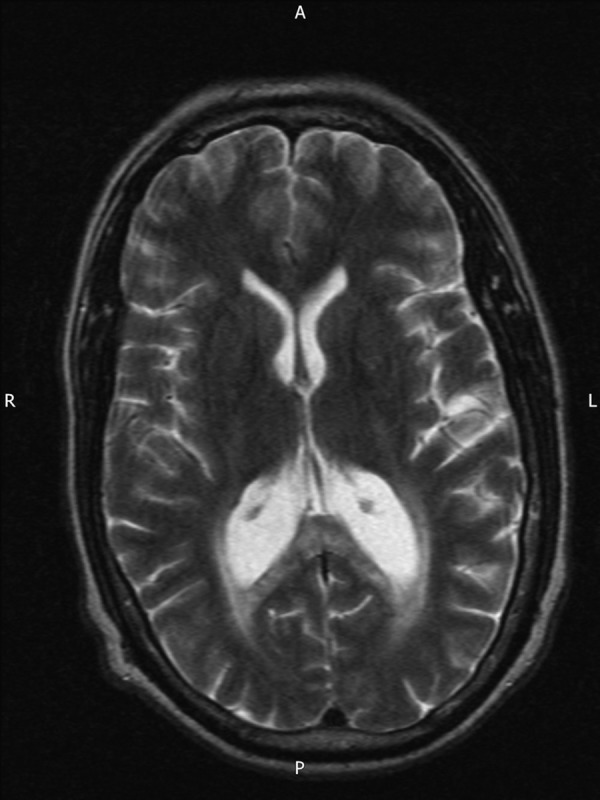
A T2-weighted axial MRI brain (patient 2), undertaken in 2013, showing areas of high signal surrounding the occipital horns of the lateral ventricle extending to the splenium of the corpus callosum.
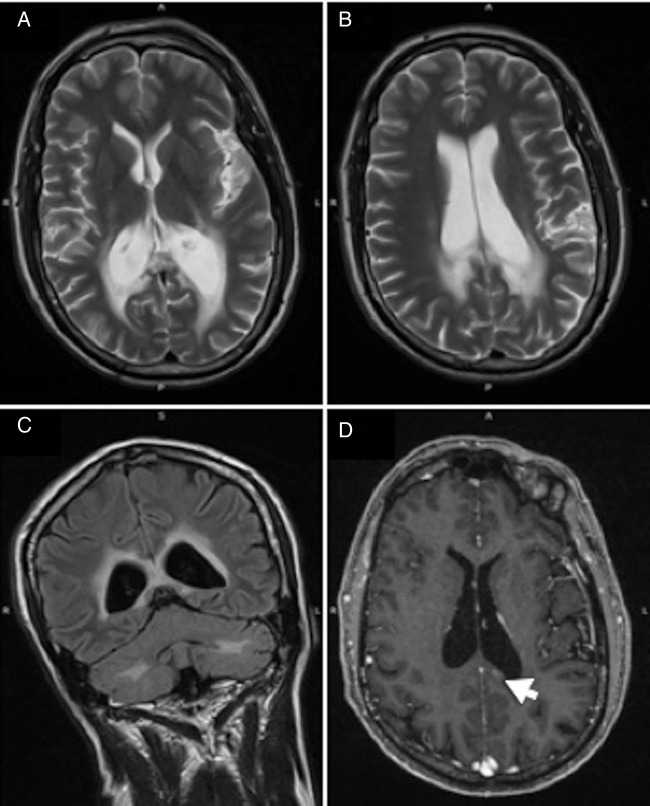
MRI brain (patient 2) undertaken in 2014: (A and B) T2-weighted axial views showing slight progression of white matter signal abnormalities. (C) Fluid-attenuated inversion recovery coronal scan with prominent periventricular rim hyper-intensity. (D) Gadolinium-enhanced T1-weighted axial scan with an area of increased enhancement (indicated by the arrow).
Similar articles
-
[Adrenomyeloneuropathy: a form of X-linked adrenoleukodystrophy. Report of a family].Neurol Neurochir Pol. 1999 Sep-Oct;33(5):1173-85. Neurol Neurochir Pol. 1999. PMID: 10672567 Polish.
-
Adrenomyeloneuropathy, a dynamic progressive disorder: brain magnetic resonance imaging of two cases.Neuroradiology. 2004 Apr;46(4):296-300. doi: 10.1007/s00234-003-1096-8. Epub 2004 Mar 4. Neuroradiology. 2004. PMID: 15007575
-
Leukodystrophies underlying cryptic spastic paraparesis: frequency and phenotype in 76 patients.Eur J Neurol. 2014 Jul;21(7):983-8. doi: 10.1111/ene.12423. Epub 2014 Apr 2. Eur J Neurol. 2014. PMID: 24698313
-
X-Linked adrenoleukodystrophy: overview and prognosis as a function of age and brain magnetic resonance imaging abnormality. A study involving 372 patients.Neuropediatrics. 2000 Oct;31(5):227-39. doi: 10.1055/s-2000-9236. Neuropediatrics. 2000. PMID: 11204280 Review.
-
Adrenomyeloneuropathy as a cause of primary adrenal insufficiency and spastic paraparesis.CMAJ. 2004 Oct 26;171(9):1073-7. doi: 10.1503/cmaj.1032006. CMAJ. 2004. PMID: 15505272 Free PMC article. Review.
Cited by
-
X-linked cerebral adrenoleukodystrophy.BMJ Case Rep. 2023 Oct 31;16(10):e237905. doi: 10.1136/bcr-2020-237905. BMJ Case Rep. 2023. PMID: 37907311
-
Management of X-linked adrenoleukodystrophy in Morocco: actual situation.BMC Res Notes. 2017 Nov 7;10(1):567. doi: 10.1186/s13104-017-2902-4. BMC Res Notes. 2017. PMID: 29116030 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources