

Prevalence of rheumatoid arthritis in low- and middle-income countries: A systematic review and analysis
- PMID: 25969732
- PMCID: PMC4416333
- DOI: 10.7189/jogh.05.010409
Prevalence of rheumatoid arthritis in low- and middle-income countries: A systematic review and analysis
Abstract
Background: Rheumatoid arthritis (RA) is an autoimmune disorder that affects the small joints of the body. It is one of the leading causes of chronic morbidity in high-income countries, but little is known about the burden of this disease in low- and middle-income countries (LMIC).
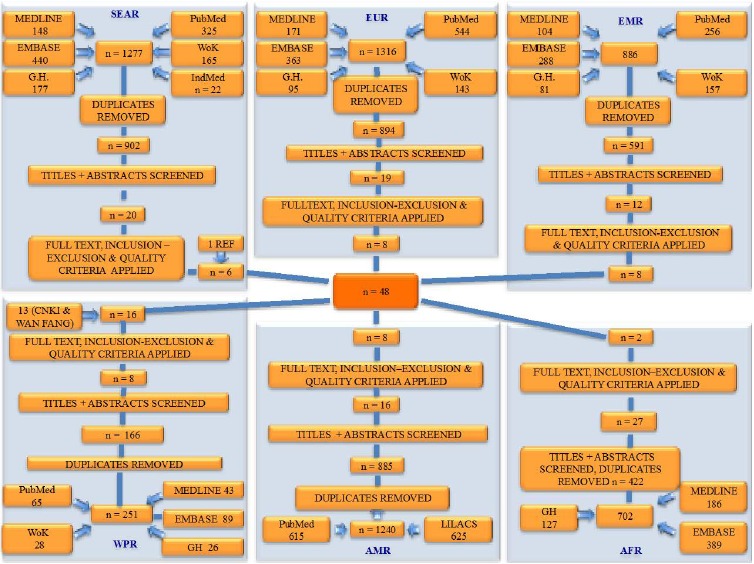
Methods: The aim of this study was to estimate the prevalence of RA in six of the World Health Organization's (WHO) regions that harbour LMIC by identifying all relevant studies in those regions. To accomplish this aim various bibliographic databases were searched: PubMed, EMBASE, Global Health, LILACS and the Chinese databases CNKI and WanFang. Studies were selected based on pre-defined inclusion criteria, including a definition of RA based on the 1987 revision of the American College of Rheumatology (ACR) definition.
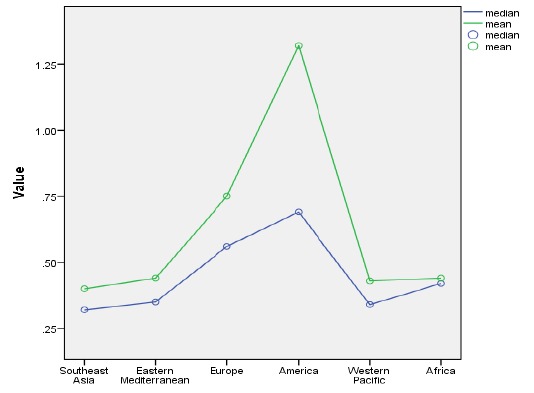
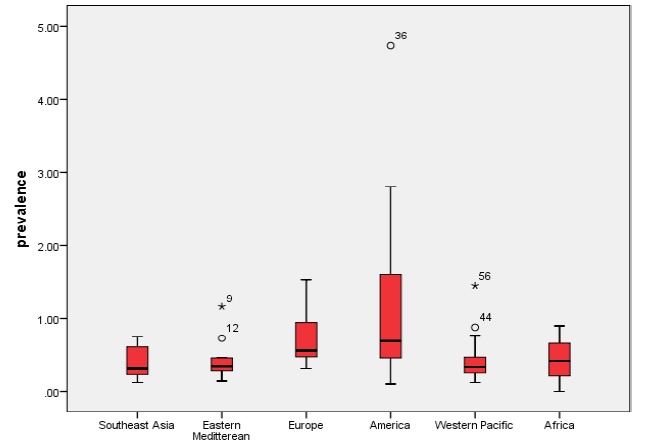
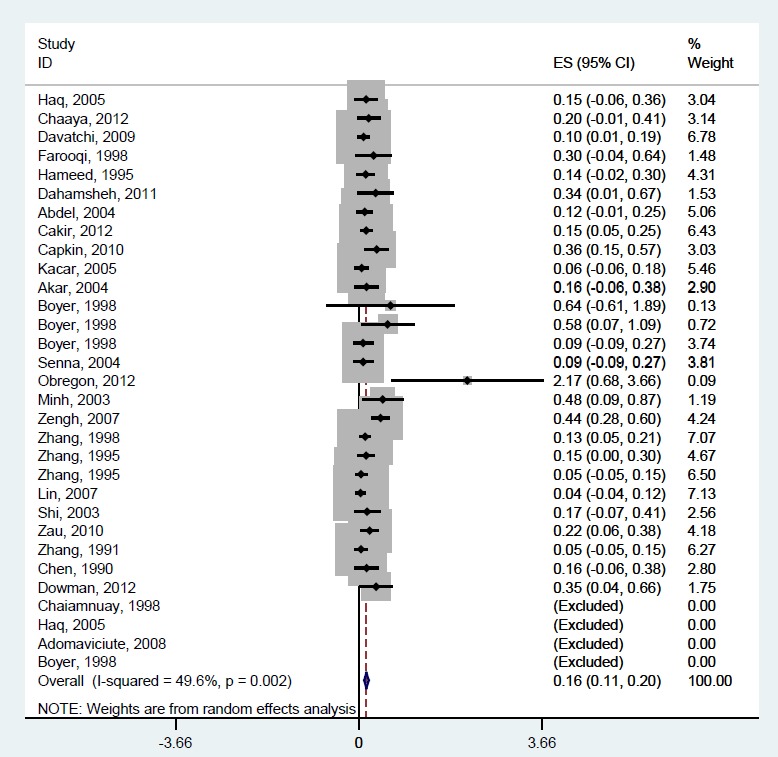
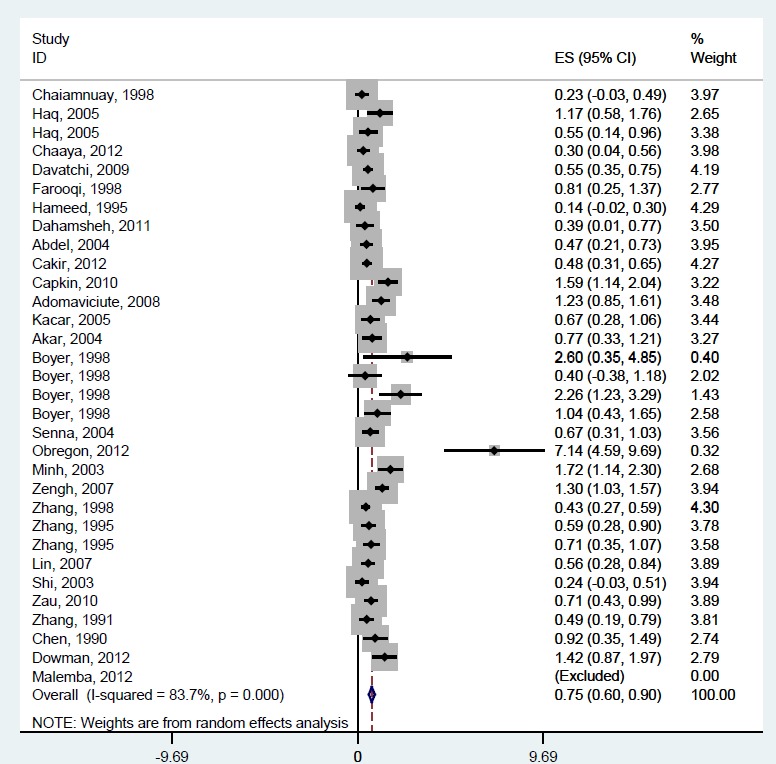
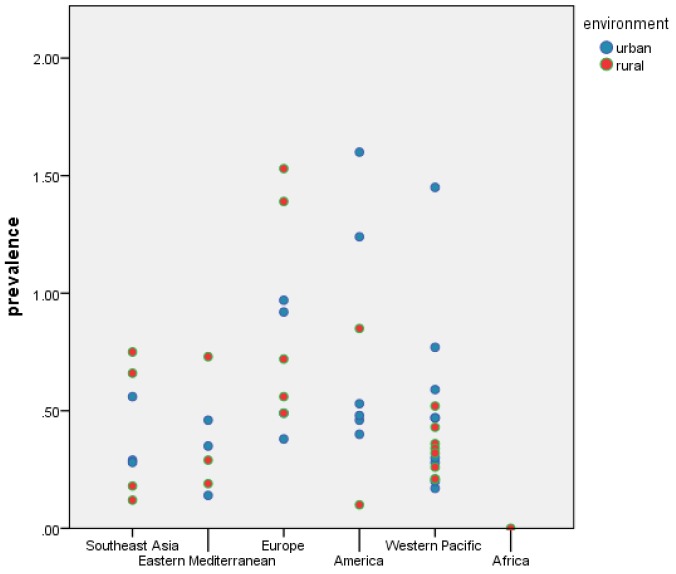
Results: Meta-estimates of regional RA prevalence rates for countries of low or middle income were 0.40% (95% CI: 0.23-0.57%) for Southeast Asian, 0.37% (95% CI: 0.23-0.51%) for Eastern Mediterranean, 0.62% (95% CI: 0.47-0.77%) for European, 1.25% (95% CI: 0.64-1.86%) for American and 0.42% (95% CI: 0.30-0.53%) for Western Pacific regions. A formal meta-analysis could not be performed for the sub-Saharan African region due to limited data. Male prevalence of RA in LMIC was 0.16% (95% CI: 0.11-0.20%) while the prevalence in women reached 0.75% (95% CI: 0.60-0.90%). This difference between males and females was statistically significant (P < 0.0001). The prevalence of RA did not differ significantly between urban and rural settings (P = 0.353). These prevalence estimates represent 2.60 (95% CI: 1.85-3.34%) million male sufferers and 12.21 (95% CI: 9.78-14.67%) million female sufferers in LMIC in the year 2000, and 3.16 (95% CI: 2.25-4.05%) million affected males and 14.87 (95% CI: 11.91-17.86%) million affected females in LMIC in the year 2010.
Conclusion: Given that majority of the world's population resides in LMIC, the number of affected people is substantial, with a projection to increase in the coming years. Therefore, policy makers and health-care providers need to plan to address a significant disease burden both socially and economically.
Figures
References
-
- United Nations. Prevention and control of non–communicable diseases: Report of the Secretary–General. New York: United Nations, 2011. Available: http://www.un.org/ga/search/view_doc.asp?symbol=A/66/83&referer=/english.... Accessed: 2 May 2014.
-
- World Health Organization. UN High Level Meeting on NCD: Summary report of the discussion at the round tables. Geneva: World Health Organization, 2011. Available: http://www.who.int/nmh/events/moscow_NCD_2011/round_tables_summary.pdf. Accessed: 2 May 2014.
LinkOut - more resources
Full Text Sources