

Direct estimates of national neonatal and child cause-specific mortality proportions in Niger by expert algorithm and physician-coded analysis of verbal autopsy interviews
- PMID: 25969734
- PMCID: PMC4416334
- DOI: 10.7189/jogh.05.010415
Direct estimates of national neonatal and child cause-specific mortality proportions in Niger by expert algorithm and physician-coded analysis of verbal autopsy interviews
Abstract
Background: This study was one of a set of verbal autopsy investigations undertaken by the WHO/UNCEF-supported Child Health Epidemiology Reference Group (CHERG) to derive direct estimates of the causes of neonatal and child deaths in high priority countries of sub-Saharan Africa. The objective of the study was to determine the cause distributions of neonatal (0-27 days) and child (1-59 months) mortality in Niger.
Methods: Verbal autopsy interviews were conducted of random samples of 453 neonatal deaths and 620 child deaths from 2007 to 2010 identified by the 2011 Niger National Mortality Survey. The cause of each death was assigned using two methods: computerized expert algorithms arranged in a hierarchy and physician completion of a death certificate for each child. The findings of the two methods were compared to each other, and plausibility checks were conducted to assess which is the preferred method. Comparison of some direct measures from this study with CHERG modeled cause of death estimates are discussed.
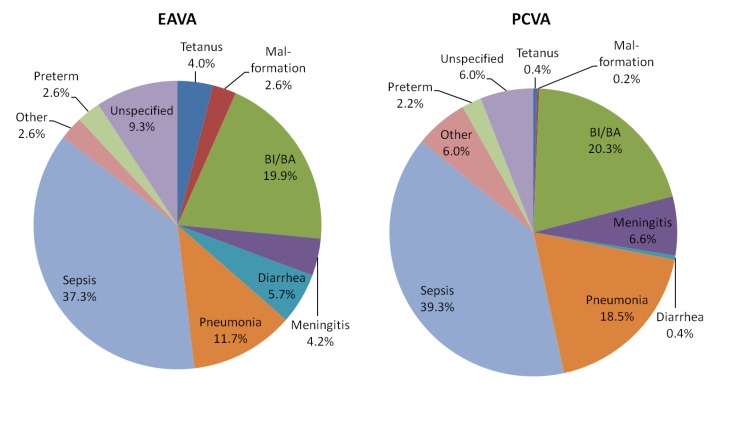
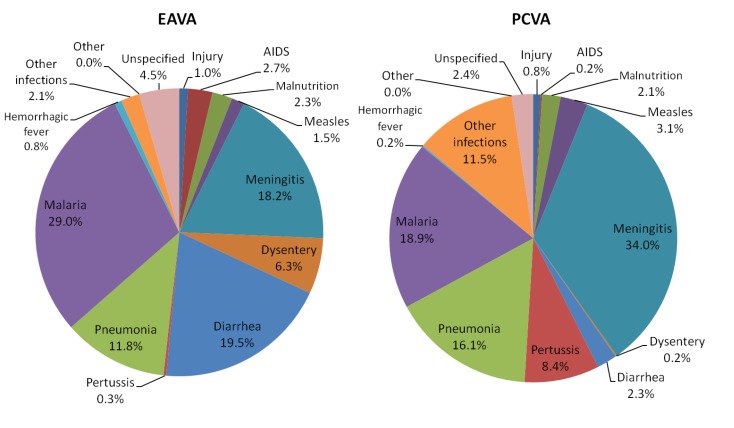
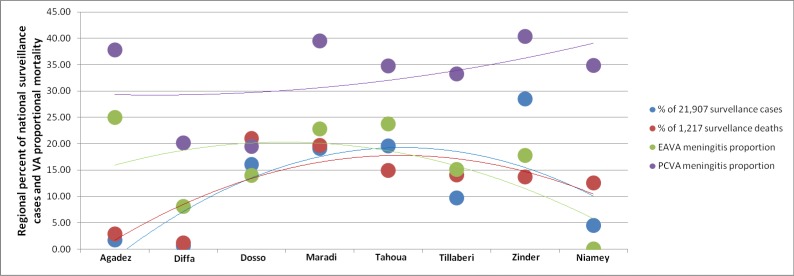
Findings: The cause distributions of neonatal deaths as determined by expert algorithms and the physician were similar, with the same top three causes by both methods and all but two other causes within one rank of each other. Although child causes of death differed more, the reasons often could be discerned by analyzing algorithmic criteria alongside the physician's application of required minimal diagnostic criteria. Including all algorithmic (primary and co-morbid) and physician (direct, underlying and contributing) diagnoses in the comparison minimized the differences, with kappa coefficients greater than 0.40 for five of 11 neonatal diagnoses and nine of 13 child diagnoses. By algorithmic diagnosis, early onset neonatal infection was significantly associated (χ(2) = 13.2, P < 0.001) with maternal infection, and the geographic distribution of child meningitis deaths closely corresponded with that for meningitis surveillance cases and deaths.
Conclusions: Verbal autopsy conducted in the context of a national mortality survey can provide useful estimates of the cause distributions of neonatal and child deaths. While the current study found reasonable agreement between the expert algorithm and physician analyses, it also demonstrated greater plausibility for two algorithmic diagnoses and validation work is needed to ascertain the findings. Direct, large-scale measurement of causes of death complement, can strengthen, and in some settings may be preferred over modeled estimates.
Figures
References
-
- El Arifeen S, Akhter T, Chowdhury HR, Rahman KM, Chowdhury EK, Alam N, et al. Causes of death in children under five years of age. Chapter 9, Bangladesh Demographic and Health Survey 2004. Dhaka, Bangladesh and Calverton, Maryland, USA: National Institute of Population Research and Training, Mitra and Associates, and ORC Macro, 2005.
-
- Gray RH. Verbal autopsy: Using interviews to determine causes of death in children. Johns Hopkins University Institute for International Programs, Occasional paper series no. 14. Baltimore: Johns Hopkins, 1991.
LinkOut - more resources
Full Text Sources
Other Literature Sources