

Randomized trial of four financial-incentive programs for smoking cessation
- PMID: 25970009
- PMCID: PMC4471993
- DOI: 10.1056/NEJMoa1414293
Randomized trial of four financial-incentive programs for smoking cessation
Abstract
Background: Financial incentives promote many health behaviors, but effective ways to deliver health incentives remain uncertain.
Methods: We randomly assigned CVS Caremark employees and their relatives and friends to one of four incentive programs or to usual care for smoking cessation. Two of the incentive programs targeted individuals, and two targeted groups of six participants. One of the individual-oriented programs and one of the group-oriented programs entailed rewards of approximately $800 for smoking cessation; the others entailed refundable deposits of $150 plus $650 in reward payments for successful participants. Usual care included informational resources and free smoking-cessation aids.
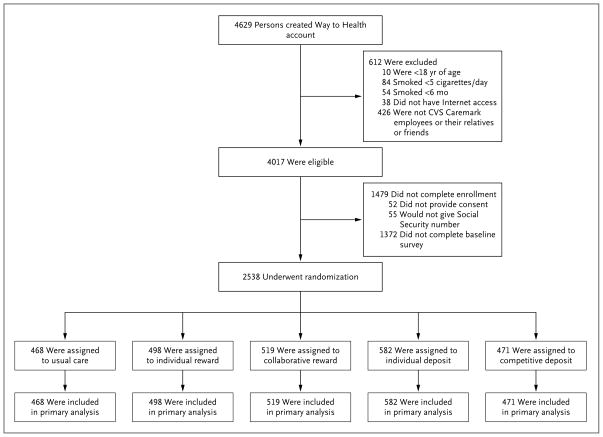
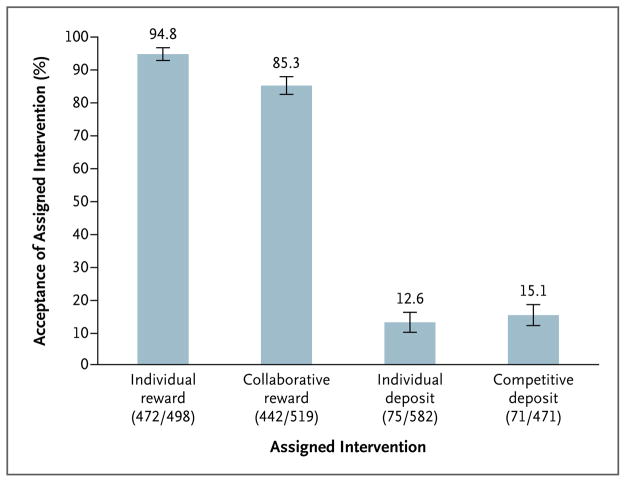
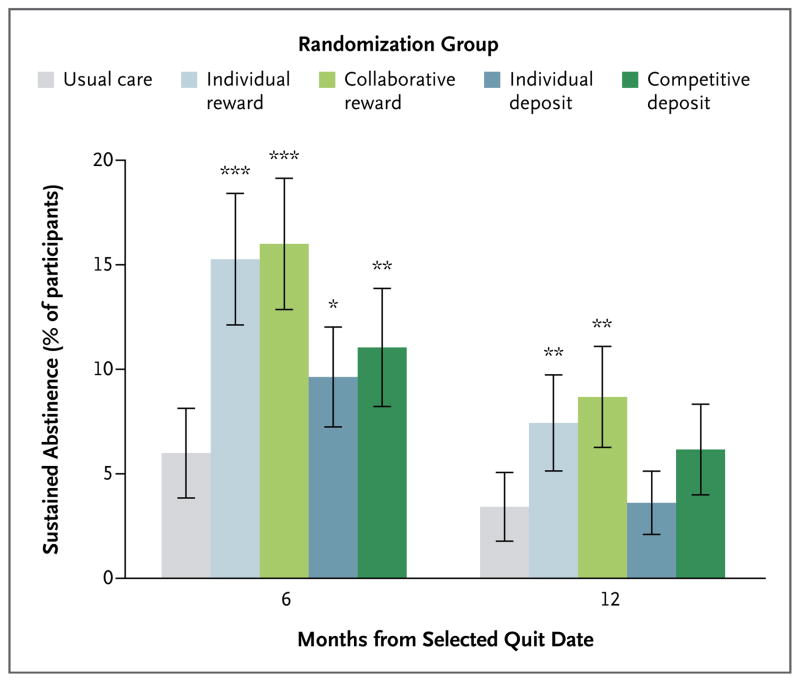
Results: Overall, 2538 participants were enrolled. Of those assigned to reward-based programs, 90.0% accepted the assignment, as compared with 13.7% of those assigned to deposit-based programs (P<0.001). In intention-to-treat analyses, rates of sustained abstinence from smoking through 6 months were higher with each of the four incentive programs (range, 9.4 to 16.0%) than with usual care (6.0%) (P<0.05 for all comparisons); the superiority of reward-based programs was sustained through 12 months. Group-oriented and individual-oriented programs were associated with similar 6-month abstinence rates (13.7% and 12.1%, respectively; P=0.29). Reward-based programs were associated with higher abstinence rates than deposit-based programs (15.7% vs. 10.2%, P<0.001). However, in instrumental-variable analyses that accounted for differential acceptance, the rate of abstinence at 6 months was 13.2 percentage points (95% confidence interval, 3.1 to 22.8) higher in the deposit-based programs than in the reward-based programs among the estimated 13.7% of the participants who would accept participation in either type of program.
Conclusions: Reward-based programs were much more commonly accepted than deposit-based programs, leading to higher rates of sustained abstinence from smoking. Group-oriented incentive programs were no more effective than individual-oriented programs. (Funded by the National Institutes of Health and CVS Caremark; ClinicalTrials.gov number, NCT01526265.).
Figures
Comment in
-
Nudging smokers.N Engl J Med. 2015 May 28;372(22):2150-1. doi: 10.1056/NEJMe1503200. Epub 2015 May 13. N Engl J Med. 2015. PMID: 25970008 No abstract available.
-
Public health: The case for pay to quit.Nature. 2015 Jul 2;523(7558):40-1. doi: 10.1038/523040a. Nature. 2015. PMID: 26135443 No abstract available.
References
-
- Higgins ST, Budney AJ, Bickel WK, Foerg FE, Donham R, Badger GJ. Incentives improve outcome in outpatient behavioral treatment of cocaine dependence. Arch Gen Psychiatry. 1994;51:568–76. - PubMed
-
- Kane RL, Johnson PE, Town RJ, Butler M. A structured review of the effect of economic incentives on consumers’ preventive behavior. Am J Prev Med. 2004;27:327–52. - PubMed
-
- Lussier JP, Heil SH, Mongeon JA, Badger GJ, Higgins ST. A meta-analysis of voucher-based reinforcement therapy for substance use disorders. Addiction. 2006;101:192–203. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical