

Chest ultrasonography in patients with HIV: a case series and review of the literature
- PMID: 25972115
- PMCID: PMC4735240
- DOI: 10.1007/s15010-015-0780-z
Chest ultrasonography in patients with HIV: a case series and review of the literature
Abstract
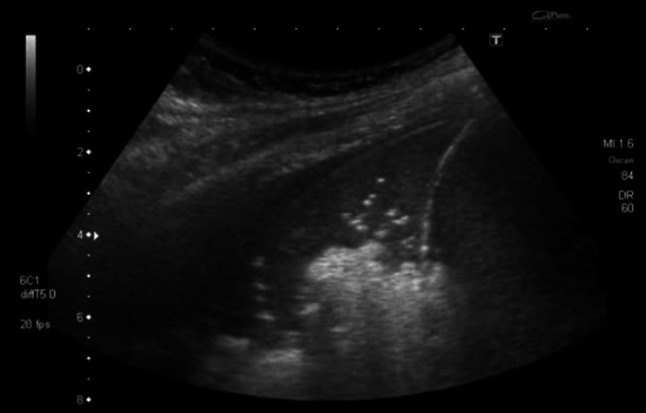
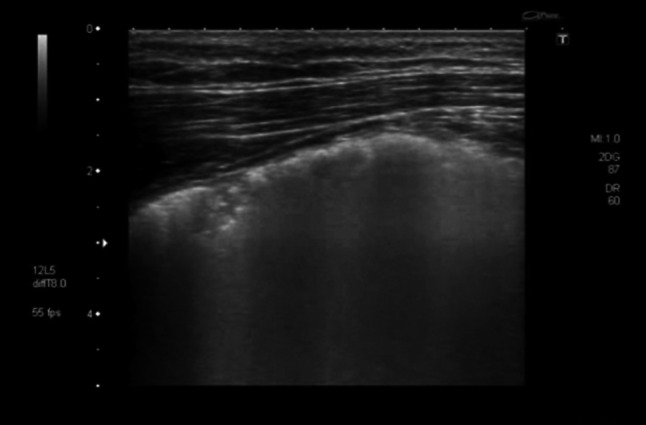
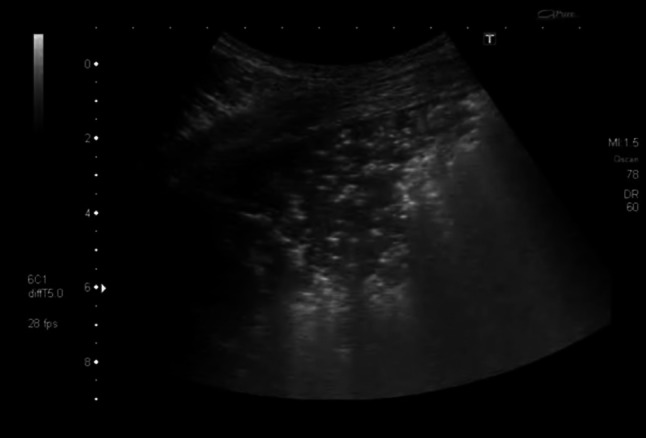
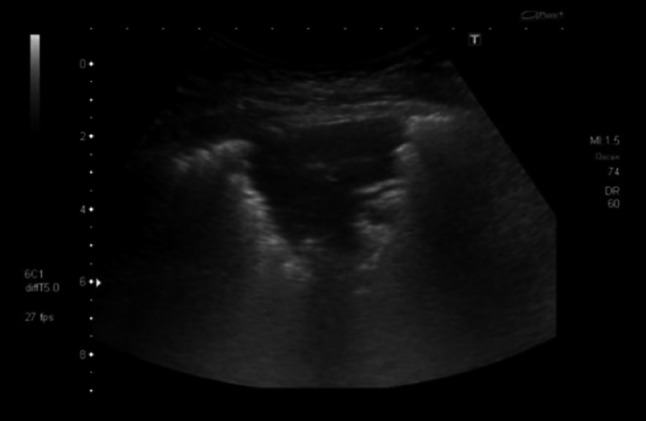
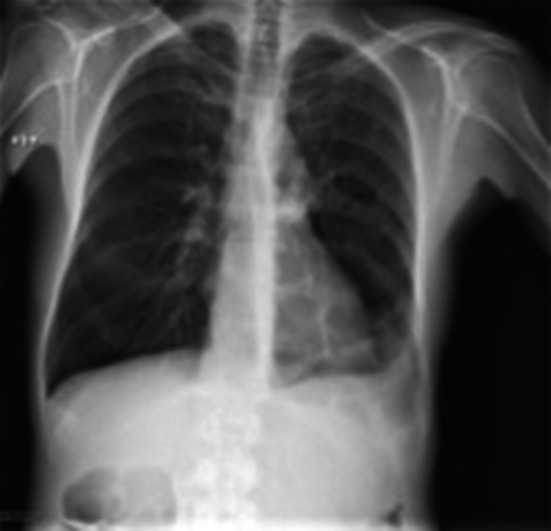
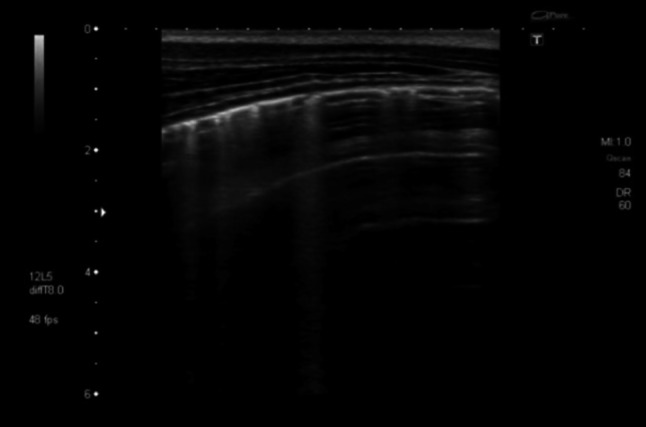
Introduction: Pulmonary disease is common in HIV-infected patients. Diagnostic means, however, are often scarce in areas where most HIV patients are living. Chest ultrasonography has recently evolved as a highly sensitive and specific imaging tool for diagnosing chest conditions such as pneumothorax, pneumonia and pulmonary edema in critically ill patients. This article addresses the issue of imaging and differentiating common pulmonary conditions in HIV-infected patients by chest ultrasonography.
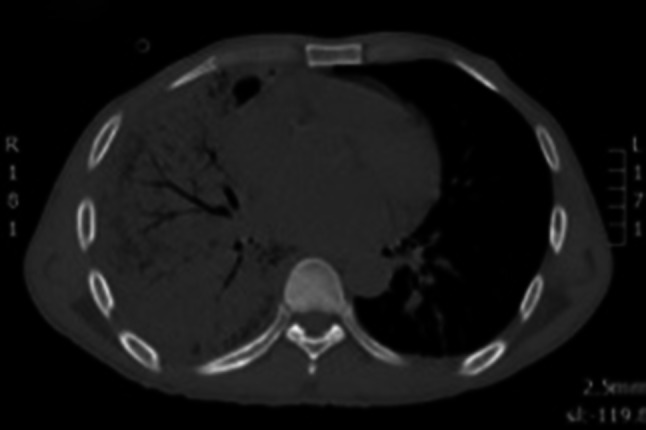
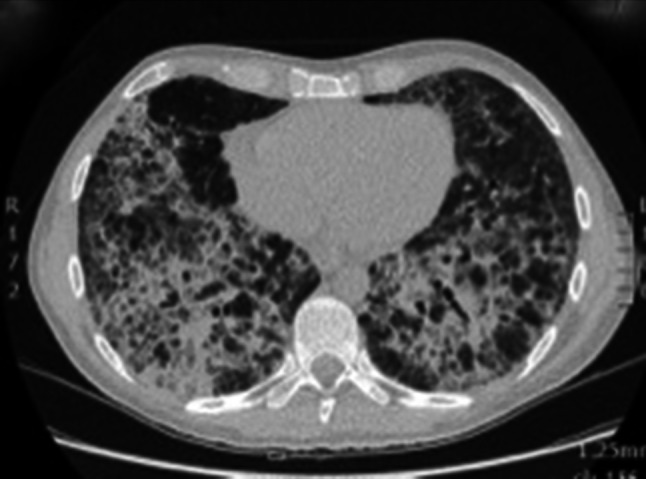
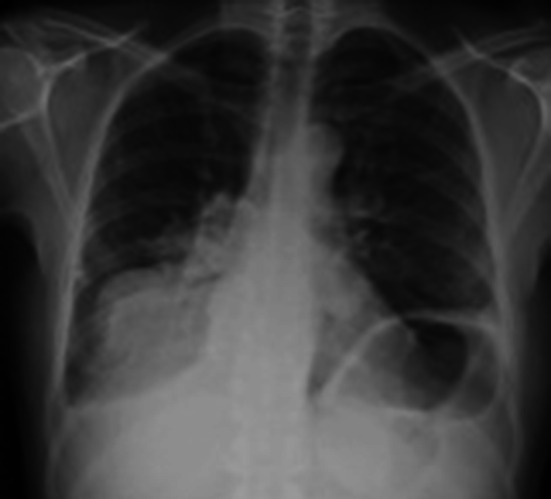
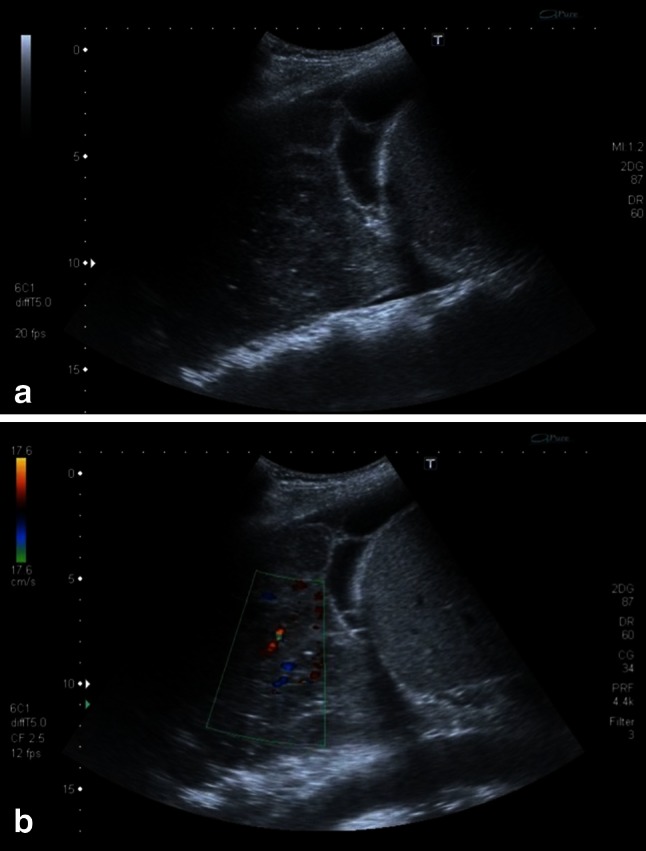
Methods: We report chest ultrasound features of five different common pulmonary diseases in HIV-infected patients (bacterial pneumonia, Pneumocystis jirovecii pneumonia, tuberculosis, cytomegalovirus pneumonia and non-Hodgkin lymphoma) and review the respective literature.
Conclusions: We observed characteristic ultrasound patterns especially in Pneumocystis jirovecii pneumonia and pulmonary lymphoma. Further exploration of chest ultrasonography in HIV-infected patients appears promising and may translate into new diagnostic approaches for pulmonary conditions in patients living with HIV.
Keywords: Chest ultrasonography; Diagnostic imaging; HIV; Infection; Lung disease; Pulmonary.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
