

Impact of Mucorales and Other Invasive Molds on Clinical Outcomes of Polymicrobial Traumatic Wound Infections
- PMID: 25972413
- PMCID: PMC4473188
- DOI: 10.1128/JCM.00835-15
Impact of Mucorales and Other Invasive Molds on Clinical Outcomes of Polymicrobial Traumatic Wound Infections
Abstract
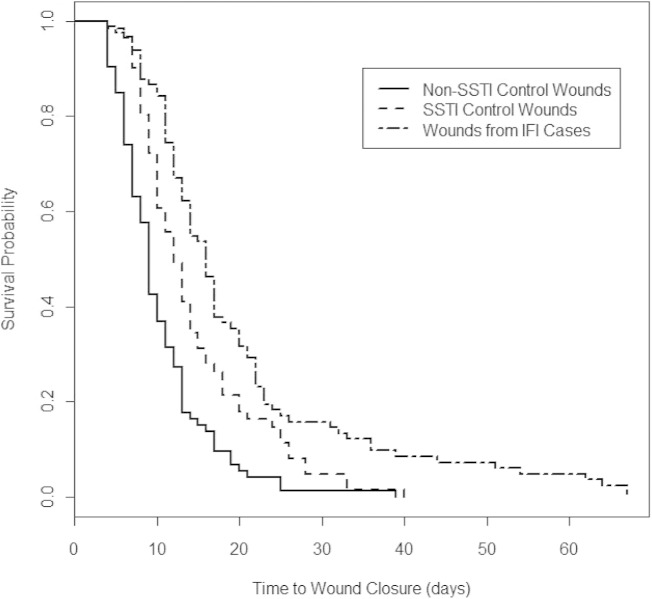
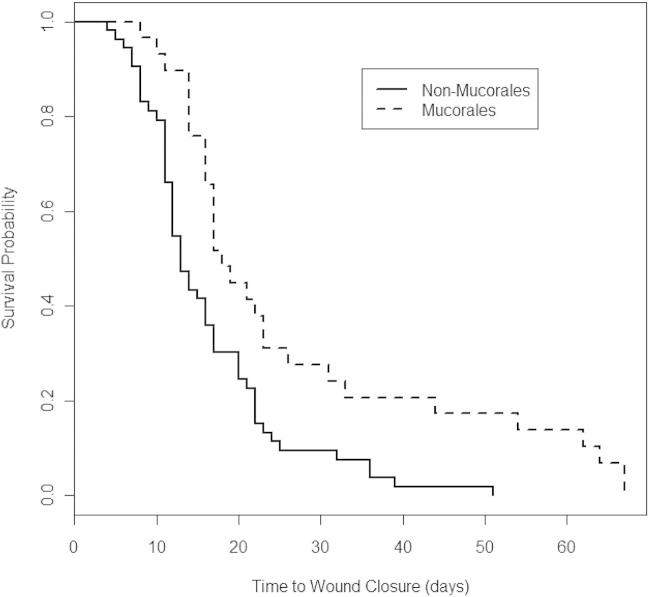
Combat trauma wounds with invasive fungal infections (IFIs) are often polymicrobial with fungal and bacterial growth, but the impact of the wound microbiology on clinical outcomes is uncertain. Our objectives were to compare the microbiological features between IFI and non-IFI wounds and evaluate whether clinical outcomes differed among IFI wounds based upon mold type. Data from U.S. military personnel injured in Afghanistan with IFI wounds were examined. Controls were matched by the pattern/severity of injury, including blood transfusion requirements. Wound closure timing was compared between IFI and non-IFI control wounds (with/without bacterial infections). IFI wound closure was also assessed according to mold species isolation. Eighty-two IFI wounds and 136 non-IFI wounds (63 with skin and soft tissue infections [SSTIs] and 73 without) were examined. The time to wound closure was longer for the IFI wounds (median, 16 days) than for the non-IFI controls with/without SSTIs (medians, 12 and 9 days, respectively; P < 0.001). The growth of multidrug-resistant Gram-negative rods was reported among 35% and 41% of the IFI and non-IFI wounds with SSTIs, respectively. Among the IFI wounds, times to wound closure were significantly longer for wounds with Mucorales growth than for wounds with non-Mucorales growth (median, 17 days versus 13 days; P < 0.01). When wounds with Mucorales and Aspergillus spp. growth were compared, there was no significant difference in wound closure timing. Trauma wounds with SSTIs were often polymicrobial, yet the presence of invasive molds (predominant types: order Mucorales, Aspergillus spp., and Fusarium spp.) significantly prolonged the time to wound closure. Overall, the times to wound closure were longest for the IFI wounds with Mucorales growth.
Copyright © 2015, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Warkentien T, Rodriguez C, Lloyd B, Wells J, Weintrob A, Dunne J, Ganesan A, Li P, Bradley W, Gaskins LJ, Seillier-Moiseiwitsch F, Murray CK, Millar EV, Keenan B, Paolino K, Fleming M, Hospenthal DR, Wortmann GW, Landrum ML, Kortepeter MG, Tribble DR. 2012. Invasive mold infections following combat-related injuries. Clin Infect Dis 55:1441–1449. doi:10.1093/cid/cis749. - DOI - PMC - PubMed
-
- Neblett Fanfair R, Benedict K, Bos J, Bennett SD, Lo Y-C, Adebanjo T, Etienne K, Deak E, Derado G, Shieh W-J, Drew C, Zaki S, Sugerman D, Gade L, Thompson EH, Sutton DA, Engelthaler DM, Schupp JM, Brandt ME, Harris JR, Lockhart SR, Turabelidze G, Park BJ. 2012. Necrotizing cutaneous mucormycosis after a tornado in Joplin, Missouri, in 2011. N Engl J Med 367:2214–2225. doi:10.1056/NEJMoa1204781. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
