

Imaging of prostate cancer with PET/CT using (18)F-Fluorocholine
- PMID: 25973332
- PMCID: PMC4396012
Imaging of prostate cancer with PET/CT using (18)F-Fluorocholine
Abstract
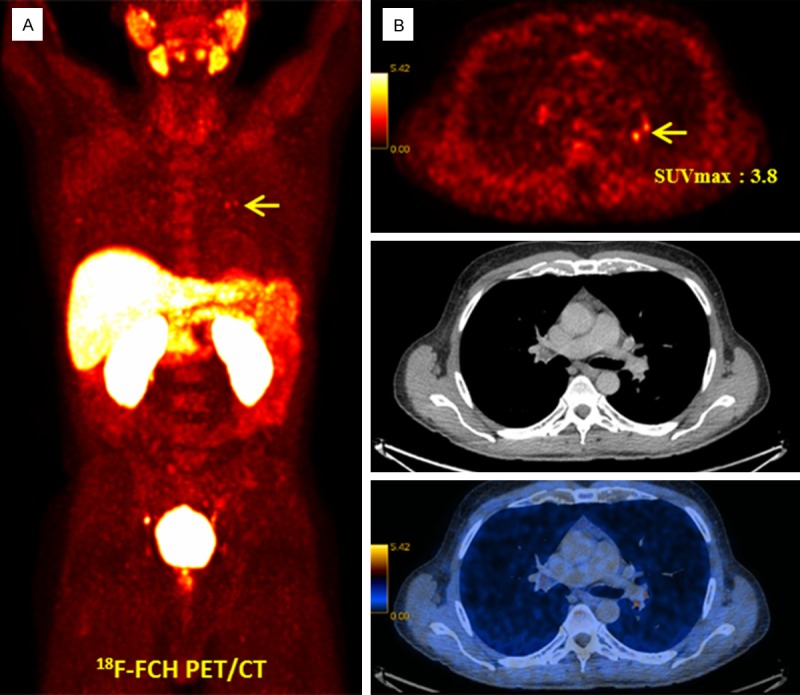
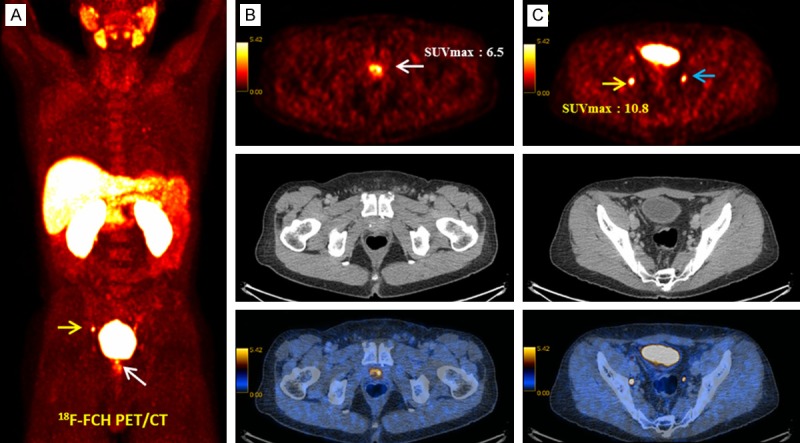
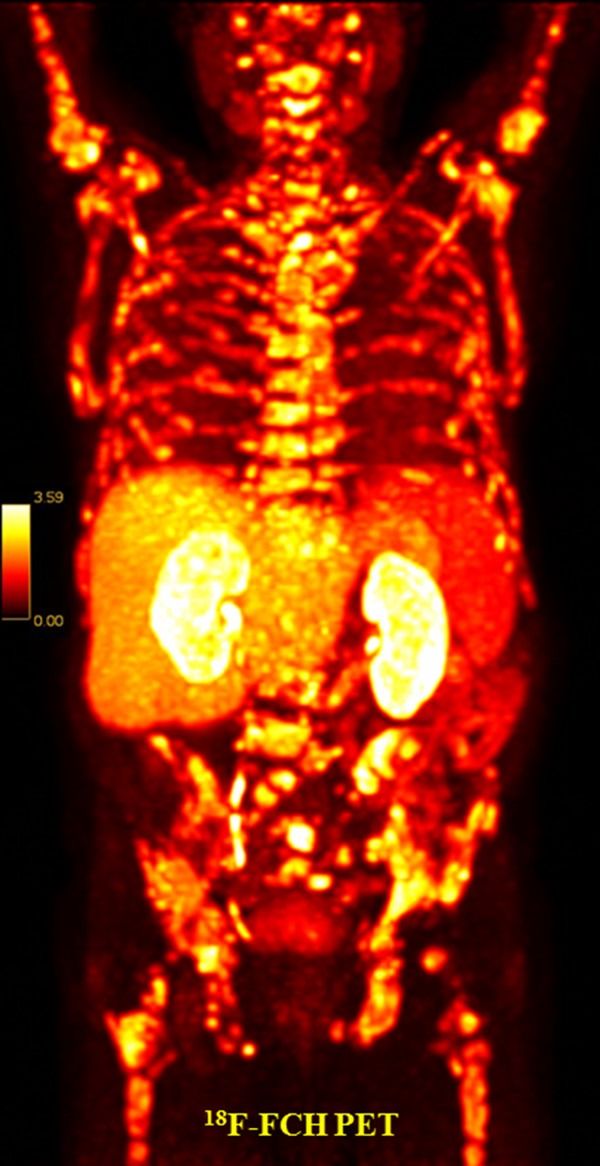
While (18)F-Fluorodeoxyglucose ((18)F-FDG) Positron-Emission Tomography (PET) has limited value in prostate cancer (PCa), it may be useful for specific subgroups of PCa patients with hormone-resistant poorly differentiated cell types. (18)F-Fluorocholine ((18)F-FCH) PET/CT has been increasingly used in primary and recurrent PCa and has been shown to add valuable information. Although there is a correlation between the foci of activity and the areas of malignancy in the prostate gland, the clinical value of (18)F-FCH is still controversial for detection of the malignant focus in the prostate. For the T-staging of PCa at diagnosis the value of (18)F-FCH is limited. This is probably due to limited resolution of PET system and positive findings in benign prostate diseases. Conversely, (18)F-FCH PET/CT is a promising imaging modality for the delineation of local and distant nodal recurrence and bone metastases and is poised to have an impact on therapy management. In this review, recent studies of (18)F-FCH PET/CT in PCa are summarized.
Keywords: 18F-Fluorocholine; PET/CT; Prostate cancer.
Figures


Similar articles
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
F-18 fluorocholine positron emission tomography- computed tomography in initial staging and recurrence evaluation of prostate carcinoma: A prospective comparative study with diffusion-weighted magnetic resonance imaging and whole-body skeletal scintigraphy.World J Nucl Med. 2021 Feb 12;20(2):156-163. doi: 10.4103/wjnm.WJNM_46_20. eCollection 2021 Apr-Jun. World J Nucl Med. 2021. PMID: 34321968 Free PMC article.
-
[18F]fluoromethylcholine (FCH) positron emission tomography/computed tomography (PET/CT) for lymph node staging of prostate cancer: a prospective study of 210 patients.BJU Int. 2012 Dec;110(11):1666-71. doi: 10.1111/j.1464-410X.2012.11150.x. Epub 2012 Apr 23. BJU Int. 2012. PMID: 22520686
-
Imaging of Prostate Cancer Using 18F-Choline PET/Computed Tomography.PET Clin. 2017 Apr;12(2):173-184. doi: 10.1016/j.cpet.2016.11.004. Epub 2017 Jan 16. PET Clin. 2017. PMID: 28267451 Review.
-
Evaluation of Prostate Cancer Bone Metastases with 18F-NaF and 18F-Fluorocholine PET/CT.J Nucl Med. 2016 Oct;57(Suppl 3):55S-60S. doi: 10.2967/jnumed.115.169730. J Nucl Med. 2016. PMID: 27694173 Review.
Cited by
-
Initial single-centre Canadian experience with 18F-fluoromethylcholine positron emission tomography-computed tomography (18F-FCH PET/CT) for biochemical recurrence in prostate cancer patients initially treated with curative intent.Can Urol Assoc J. 2017 Jan-Feb;11(1-2):47-52. doi: 10.5489/cuaj.4068. Can Urol Assoc J. 2017. PMID: 28443145 Free PMC article.
-
Therapy assessment of bone metastatic disease in the era of 223radium.Eur J Nucl Med Mol Imaging. 2017 Aug;44(Suppl 1):84-96. doi: 10.1007/s00259-017-3734-0. Epub 2017 May 31. Eur J Nucl Med Mol Imaging. 2017. PMID: 28567494 Review.
-
A PSMA Ligand Labeled with Cobalt-55 for PET Imaging of Prostate Cancer.Mol Imaging Biol. 2017 Dec;19(6):915-922. doi: 10.1007/s11307-017-1121-7. Mol Imaging Biol. 2017. PMID: 28924629
-
Metabolomics approaches in pancreatic adenocarcinoma: tumor metabolism profiling predicts clinical outcome of patients.BMC Med. 2017 Mar 16;15(1):56. doi: 10.1186/s12916-017-0810-z. BMC Med. 2017. PMID: 28298227 Free PMC article.
-
Radiopharmaceuticals for Skeletal Muscle PET Imaging.Int J Mol Sci. 2024 Apr 29;25(9):4860. doi: 10.3390/ijms25094860. Int J Mol Sci. 2024. PMID: 38732077 Free PMC article. Review.
References
-
- Stamey TA, Caldwell M, McNeal JE, Nolley R, Hemenez M, Downs J. The prostate specific antigen era in the United States is over for prostate cancer: what happened in the last 20 years? J Urol. 2004;172:1297–1301. - PubMed
-
- Oehr P, Bouchelouche K. Imaging of prostate cancer. Curr Opin Oncol. 2007;19:259–264. - PubMed
-
- Morris MJ, Akhurst T, Osman I, Nunez R, Macapinlac H, Siedlecki K, Verbel D, Schwartz L, Larson SM, Scher HI. Fluorinated deoxyglucose positron emission tomography imaging in progressive metastatic prostate cancer. Urology. 2002;59:913–918. - PubMed
-
- Sanz G, Robles JE, Gimenez M, Arocena J, Sanchez D, Rodriguez-Rubio F, Rosell D, Richter JA, Berian JM. Positron emission tomography with 18fluorine-labelled deoxyglucose: utility in localized and advanced prostate cancer. BJU Int. 1999;84:1028–1031. - PubMed
-
- Minamimoto R, Uemura H, Sano F, Terao H, Nagashima Y, Yamanaka S, Shizukuishi K, Tateishi U, Kubota Y, Inoue T. The potential of FDG-PET/CT for detecting prostate cancer in patients with an elevated serum PSA level. Ann Nucl Med. 2011;25:21–27. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources