

Anatomic Double-Bundle Reinsertion After Acute Proximal Anterior Cruciate Ligament Injury Using Knotless PushLock Anchors
- PMID: 25973366
- PMCID: PMC4427636
- DOI: 10.1016/j.eats.2014.09.007
Anatomic Double-Bundle Reinsertion After Acute Proximal Anterior Cruciate Ligament Injury Using Knotless PushLock Anchors
Abstract
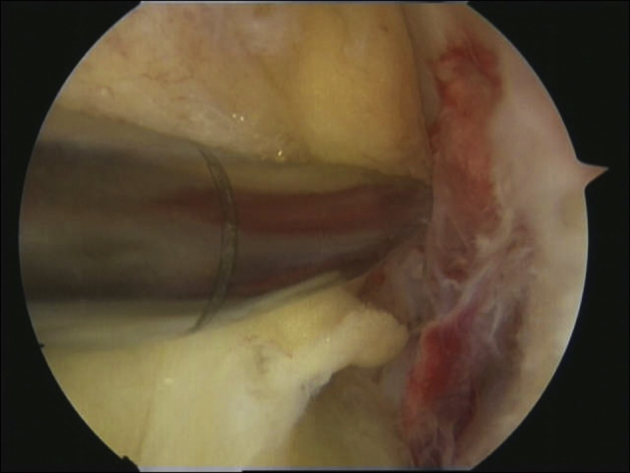
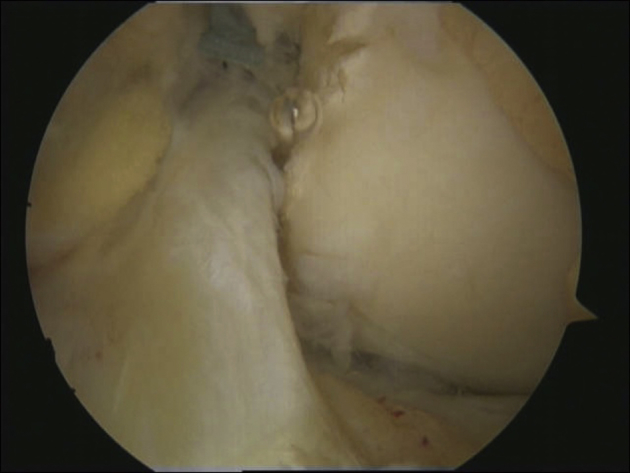
Direct anterior cruciate ligament (ACL) repair has been described with different suture techniques after acute ACL injury, but these procedures showed high failure rates. Recent studies, however, led to a better understanding of the biology of primary ACL healing. This article describes a novel technique combining the "healing response technique" with primary anatomic double-bundle ACL reinsertion after an acute proximal ACL tear using nonabsorbable No. 2 FiberWire (Arthrex, Naples, FL) and PushLock knotless suture anchors (Arthrex). We recommend this technique for patients with acute proximal avulsion-type ACL injuries. Postoperatively, we recommend a knee brace locked in full extension for at least 4 weeks to ensure adequate immobilization and then to increase knee flexion slowly over the next 4 weeks for subsequent healing of the ACL repair. Our technique combines anatomic positioning and reinsertion of the ACL bundles with microfracturing of the region delivering stem cells and growth factors to the repaired ACL, creating optimal conditions for the healing period. In certain cases this technique might be an alternative to conventional ACL reconstruction with autograft or allograft tendons.
Figures












References
-
- Murawski C.D., van Eck C.F., Irrgang J.J., Tashman S., Fu F.H. Operative treatment of primary anterior cruciate ligament rupture in adults. J Bone Joint Surg Am. 2014;96:685–694. - PubMed
-
- Strand T., Molster A., Hordvik M., Krukhaug Y. Long-term follow-up after primary repair of the anterior cruciate ligament: Clinical and radiological evaluation 15-23 years postoperatively. Arch Orthop Trauma Surg. 2005;125:217–221. - PubMed
-
- Steadman J.R., Matheny L.M., Briggs K.K., Rodkey W.G., Carreira D.S. Outcomes following healing response in older, active patients: A primary anterior cruciate ligament repair technique. J Knee Surg. 2012;25:255–260. - PubMed
-
- Steadman J.R., Cameron-Donaldson M.L., Briggs K.K., Rodkey W.G. A minimally invasive technique (“healing response”) to treat proximal ACL injuries in skeletally immature athletes. J Knee Surg. 2006;19:8–13. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
