

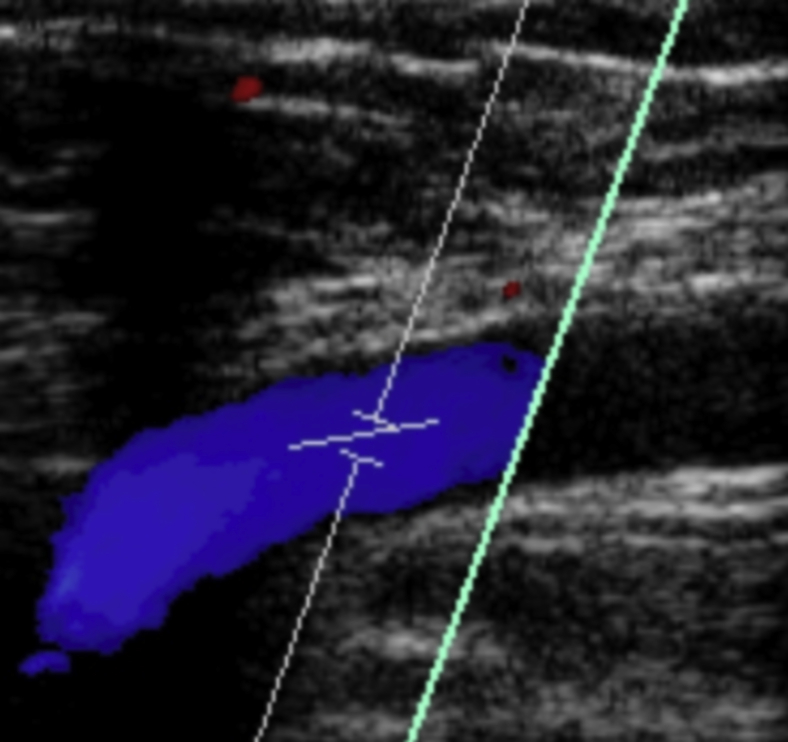
Acetabular paralabral cyst: an unusual cause of femoral vein compression
- PMID: 25973371
- PMCID: PMC4427643
- DOI: 10.1016/j.eats.2014.10.003
Acetabular paralabral cyst: an unusual cause of femoral vein compression
Abstract
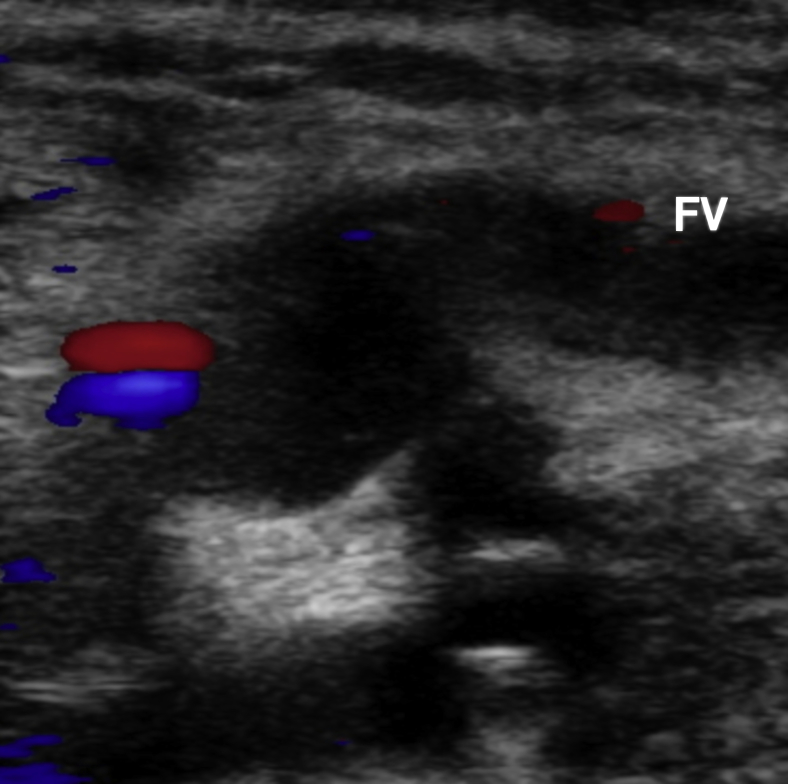
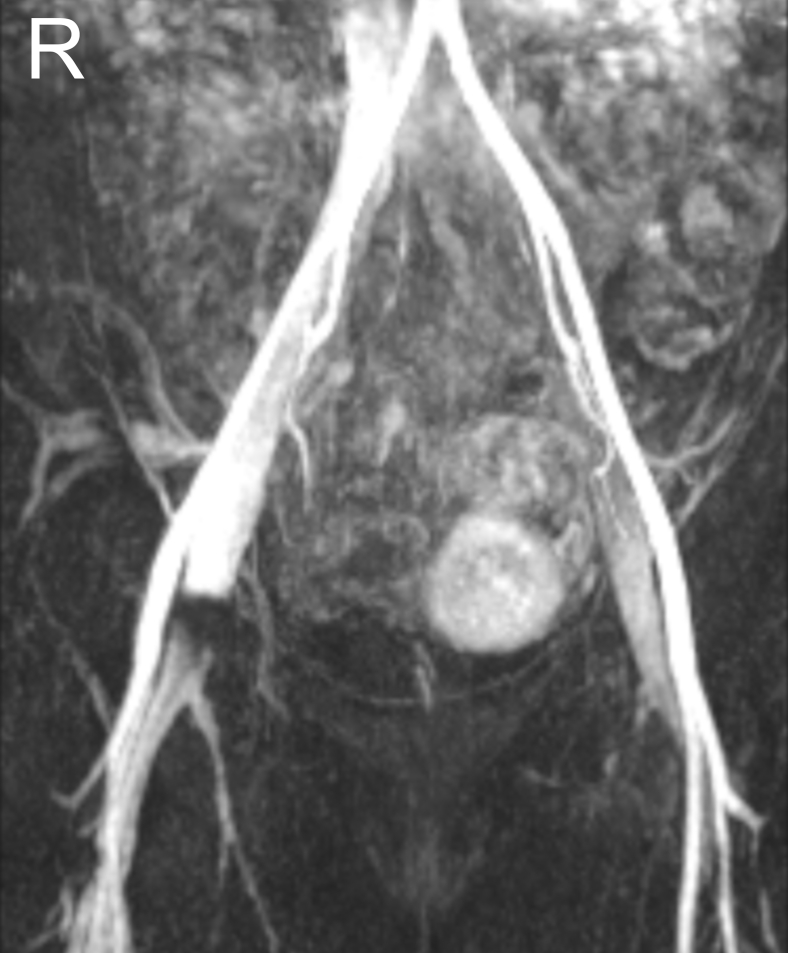
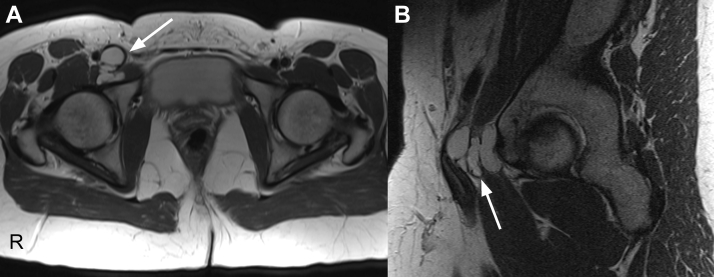
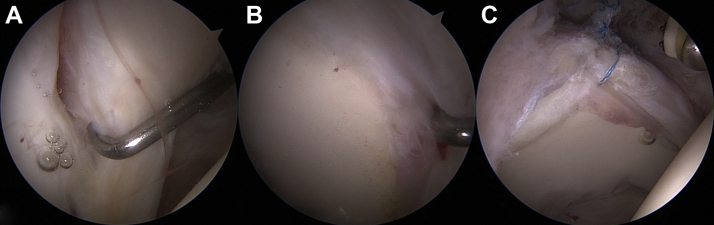
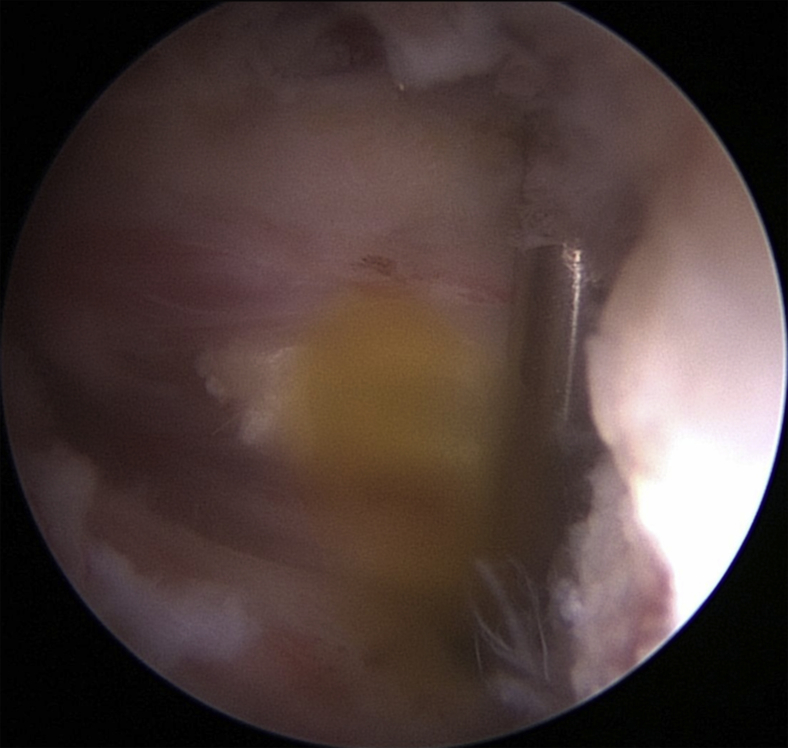
Acetabular labral tears are a known cause of hip pain in the young, active patient. Labral tears can be due to trauma, femoroacetabular impingement, capsular laxity, dysplasia, and degenerative pathology. Paralabral cysts are relatively common in association with labral tears of the hip, with cysts seen on magnetic resonance imaging studies in as many as 50% to 70% of patients with labral tears. In some cases the cysts can become sizeable and cause neurovascular compression. Nonoperative interventions for the management of paralabral cysts in the shoulder and knee have shown high recurrence rates. In the shoulder and knee, arthroscopic debridement of paralabral cysts has shown good results with lower recurrence rates and resolution of neurovascular function. In the hip there is limited literature regarding surgical management of paralabral cysts. We present a surgical technique for arthroscopic decompression of acetabular paralabral cysts combined with labral repair.
Figures

References
-
- Beaulé P.E., O’Neill M., Rakhra K. Acetabular labral tears. J Bone Joint Surg Am. 2009;91:701–710. - PubMed
-
- Ilizaliturri V.M., Jr., Gonzalez-Gutierrez B., Gonzalez-Ugalde H., Camacho-Galindo J. Hip arthroscopy after traumatic hip dislocation. Am J Sports Med. 2011;39:50S–57S. (suppl) - PubMed
-
- Philippon M.J., Kuppersmith D.A., Wolff A.B., Briggs K.K. Arthroscopic findings following traumatic hip dislocation in 14 professional athletes. Arthroscopy. 2009;25:169–174. - PubMed
-
- Shindle M.K., Kelly B.T., Lane C.G., Kelley B., Warren R.F., Voos J.E. Anterior labral tears with posterior hip subluxation or dislocation. Arthroscopy. 2008;24:e33–e34. (abstr)
LinkOut - more resources
Full Text Sources
Other Literature Sources
