

Sudomotor innervation in transthyretin amyloid neuropathy: Pathology and functional correlates
- PMID: 25973863
- PMCID: PMC5034810
- DOI: 10.1002/ana.24438
Sudomotor innervation in transthyretin amyloid neuropathy: Pathology and functional correlates
Abstract
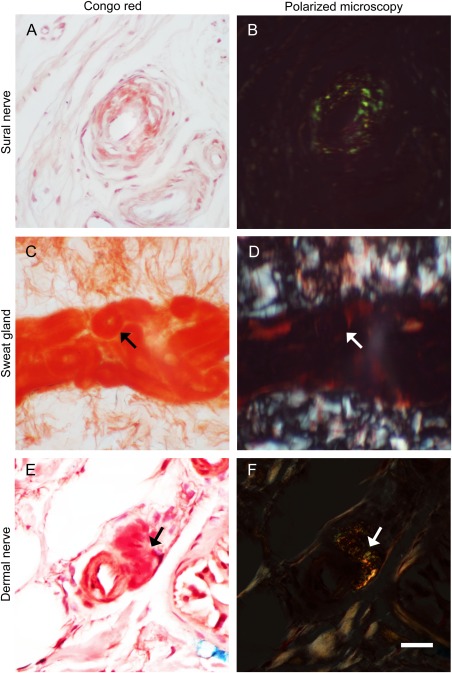
Objective: Autonomic neuropathy is a major component of familial amyloid polyneuropathy (FAP) due to mutated transthyretin, with sudomotor failure as a common manifestation. This study aimed to investigate the pathology and clinical significance of sudomotor denervation.
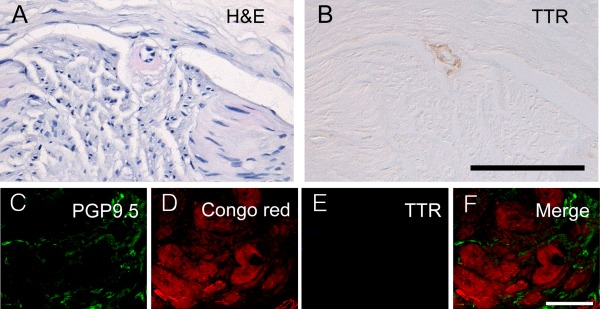
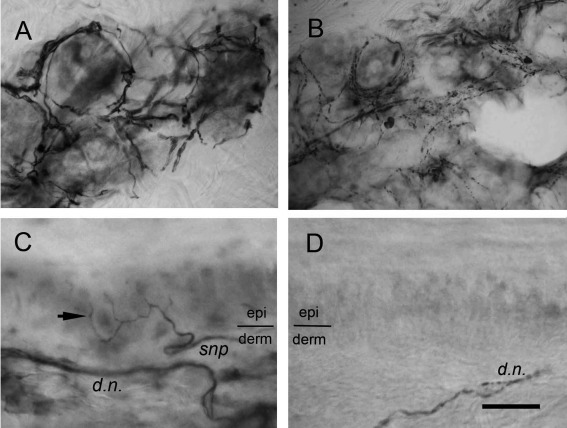
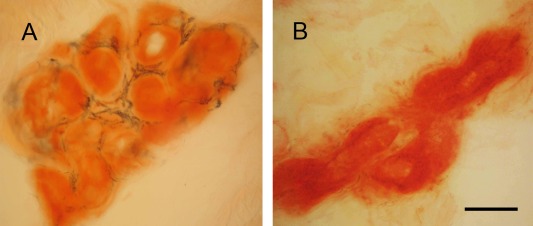
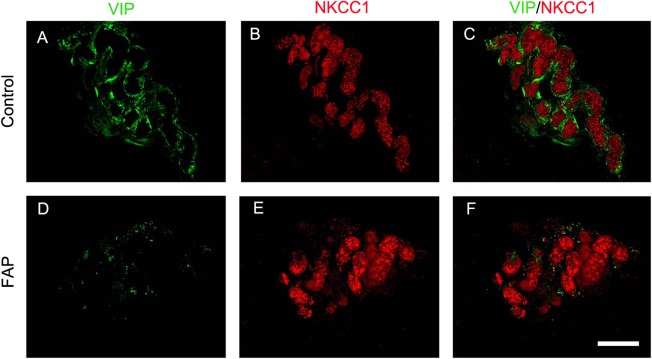
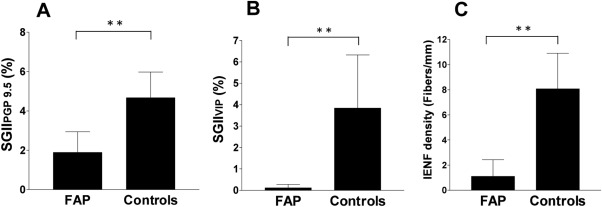
Methods: Skin biopsies were performed on the distal leg of FAP patients with a follow-up duration of 3.8 ± 1.6 years. Sudomotor innervation was stained with 2 markers: protein gene product 9.5 (PGP 9.5), a general neuronal marker, and vasoactive intestinal peptide (VIP), a sudomotor nerve functional marker, followed by quantitation according to sweat gland innervation index (SGII) for PGP 9.5 (SGIIPGP 9.5) and VIP (SGIIVIP).
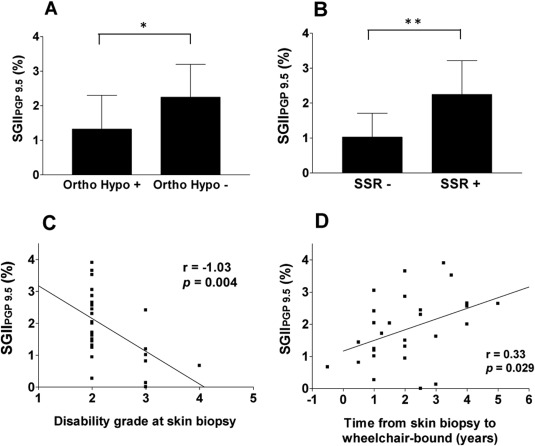
Results: There were 28 patients (25 men) with Ala97Ser transthyretin and late onset (59.9 ± 6.0 years) disabling neuropathy. Autonomic symptoms were present in 22 patients (78.6%) at the time of skin biopsy. The SGIIPGP 9.5 and SGIIVIP of FAP patients were significantly lower than those of age- and gender-matched controls. The reduction of SGIIVIP was more severe than that of SGIIPGP 9.5 (p = 0.002). Patients with orthostatic hypotension or absent sympathetic skin response at palms were associated with lower SGIIPGP 9.5 (p = 0.019 and 0.002, respectively). SGIIPGP 9.5 was negatively correlated with the disability grade at the time of skin biopsy (p = 0.004), and was positively correlated with the interval from the time of skin biopsy to the time of wheelchair usage (p = 0.029).
Interpretation: This study documented the pathological evidence of sudomotor denervation in FAP. SGIIPGP 9.5 was functionally correlated with autonomic symptoms, autonomic tests, ambulation status, and progression of disability.
© 2015 The Authors Annals of Neurology published by Wiley Periodicals, Inc. on behalf of American Neurological Association.
Figures
Similar articles
-
Skin nerve pathology: Biomarkers of premanifest and manifest amyloid neuropathy.Ann Neurol. 2019 Apr;85(4):560-573. doi: 10.1002/ana.25433. Ann Neurol. 2019. PMID: 30737830
-
Cutaneous nerve biomarkers in transthyretin familial amyloid polyneuropathy.Ann Neurol. 2017 Jul;82(1):44-56. doi: 10.1002/ana.24972. Epub 2017 Jun 20. Ann Neurol. 2017. PMID: 28598015
-
Clinical presentations and skin denervation in amyloid neuropathy due to transthyretin Ala97Ser.Neurology. 2010 Aug 10;75(6):532-8. doi: 10.1212/WNL.0b013e3181ec7fda. Neurology. 2010. PMID: 20697105
-
Cutaneous Manifestations of Familial Transthyretin Amyloid Polyneuropathy.Am J Dermatopathol. 2016 Oct;38(10):719-25. doi: 10.1097/DAD.0000000000000501. Am J Dermatopathol. 2016. PMID: 26959691 Review.
-
Transthyretin Amyloid Neuropathy: The Schwann Cell Hypothesis.Adv Exp Med Biol. 2019;1190:371-378. doi: 10.1007/978-981-32-9636-7_24. Adv Exp Med Biol. 2019. PMID: 31760657 Review.
Cited by
-
Evidence of neurophysiological improvement of early manifestations of small-fiber dysfunction after liver transplantation in a patient with familial amyloid neuropathy.Clin Neurophysiol Pract. 2018 Feb 17;3:40-44. doi: 10.1016/j.cnp.2018.01.002. eCollection 2018. Clin Neurophysiol Pract. 2018. PMID: 30215006 Free PMC article.
-
Trial design and rationale for APOLLO, a Phase 3, placebo-controlled study of patisiran in patients with hereditary ATTR amyloidosis with polyneuropathy.BMC Neurol. 2017 Sep 11;17(1):181. doi: 10.1186/s12883-017-0948-5. BMC Neurol. 2017. PMID: 28893208 Free PMC article. Clinical Trial.
-
Ala97Ser transthyretin amyloidosis-associated polyneuropathy, clinical and neurophysiological profiles in a Thai cohort.BMC Neurol. 2021 May 22;21(1):206. doi: 10.1186/s12883-021-02243-3. BMC Neurol. 2021. PMID: 34022837 Free PMC article.
-
Cardiac and peripheral vasomotor autonomic functions in late-onset transthyretin Val30Met familial amyloid polyneuropathy.J Neurol. 2017 Nov;264(11):2293-2302. doi: 10.1007/s00415-017-8629-2. Epub 2017 Oct 5. J Neurol. 2017. PMID: 28983659
-
A Missense Variant p.Ala117Ser in the Transthyretin Gene of a Han Chinese Family with Familial Amyloid Polyneuropathy.Mol Neurobiol. 2018 Jun;55(6):4911-4917. doi: 10.1007/s12035-017-0694-0. Epub 2017 Jul 31. Mol Neurobiol. 2018. PMID: 28762097
References
-
- Plante‐Bordeneuve V, Said G. Familial amyloid polyneuropathy. Lancet Neurol 2011;10:1086–1097. - PubMed
-
- Ando Y, Nakamura M, Araki S. Transthyretin‐related familial amyloidotic polyneuropathy. Arch Neurol 2005;62:1057–1062. - PubMed
-
- Ikeda S, Nakazato M, Ando Y, Sobue G. Familial transthyretin‐type amyloid polyneuropathy in Japan: clinical and genetic heterogeneity. Neurology 2002;58:1001–1007. - PubMed
-
- Yang NC, Lee MJ, Chao CC, et al. Clinical presentations and skin denervation in amyloid neuropathy due to transthyretin Ala97ser. Neurology 2010;75:532–538. - PubMed
-
- Freeman R. Autonomic peripheral neuropathy. Lancet 2005;365:1259–1270. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
