

When getting there is not enough: a nationwide cross-sectional study of 998 maternal deaths and 1451 near-misses in public tertiary hospitals in a low-income country
- PMID: 25974281
- PMCID: PMC5016783
- DOI: 10.1111/1471-0528.13450
When getting there is not enough: a nationwide cross-sectional study of 998 maternal deaths and 1451 near-misses in public tertiary hospitals in a low-income country
Abstract
Objective: To investigate the burden and causes of life-threatening maternal complications and the quality of emergency obstetric care in Nigerian public tertiary hospitals.
Design: Nationwide cross-sectional study.
Setting: Forty-two tertiary hospitals.
Population: Women admitted for pregnancy, childbirth and puerperal complications.
Methods: All cases of severe maternal outcome (SMO: maternal near-miss or maternal death) were prospectively identified using the WHO criteria over a 1-year period.
Main outcome measures: Incidence and causes of SMO, health service events, case fatality rate, and mortality index (% of maternal death/SMO).
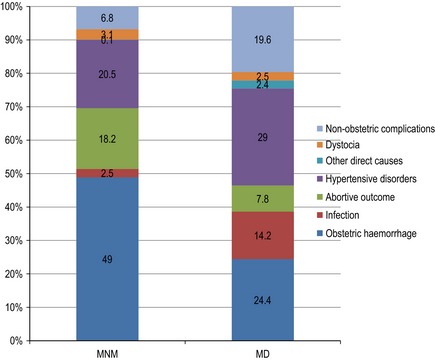
Results: Participating hospitals recorded 91 724 live births and 5910 stillbirths. A total of 2449 women had an SMO, including 1451 near-misses and 998 maternal deaths (2.7, 1.6 and 1.1% of live births, respectively). The majority (91.8%) of SMO cases were admitted in critical condition. Leading causes of SMO were pre-eclampsia/eclampsia (23.4%) and postpartum haemorrhage (14.4%). The overall mortality index for life-threatening conditions was 40.8%. For all SMOs, the median time between diagnosis and critical intervention was 60 minutes (IQR: 21-215 minutes) but in 21.9% of cases, it was over 4 hours. Late presentation (35.3%), lack of health insurance (17.5%) and non-availability of blood/blood products (12.7%) were the most frequent problems associated with deficiencies in care.
Conclusions: Improving the chances of maternal survival would not only require timely application of life-saving interventions but also their safe, efficient and equitable use. Maternal mortality reduction strategies in Nigeria should address the deficiencies identified in tertiary hospital care and prioritise the prevention of severe complications at lower levels of care.
Tweetable abstract: Of 998 maternal deaths and 1451 near-misses reported in a network of 42 Nigerian tertiary hospitals in 1 year.
Keywords: Clinical audit; WHO near-miss criteria; maternal death; maternal near miss; quality of care; severe acute maternal morbidity.
© 2015 World Health Organization; licensed by John Wiley & Sons Ltd on behalf of Royal College of Obstetricians and Gynaecologists.
Figures
Comment in
-
We can eliminate maternal deaths in resource-poor countries.BJOG. 2016 May;123(6):939. doi: 10.1111/1471-0528.13504. Epub 2015 Jul 3. BJOG. 2016. PMID: 26138097 No abstract available.
References
-
- WHO, UNICEF, UNFPA, The World Bank . Trends in maternal mortality: 1990 to 2013. Estimates by WHO, UNICEF, UNFPA, The World Bank and the United Nations Population Division. Geneva: WHO, 2014.
-
- Wang W, Alva S, Wang S, Fort A. Levels and Trends in the Use of Maternal Health Services in Developing Countries. DHS Comparative Reports No. 26. Calverton, MD: ICF Macro, 2011.
-
- Montoya A, Calvert C, Filippi V. Explaining differences in maternal mortality levels in sub‐Saharan African hospitals: a systematic review and meta‐analysis. Int Health 2014;6:12–22. - PubMed
-
- Tunçalp Ö, Hindin MJ, Adu‐Bonsaffoh K, Adanu RM. Assessment of maternal near‐miss and quality of care in a hospital‐based study in Accra, Ghana. Int J Gynaecol Obstet 2013;123:58–63. - PubMed
-
- Oladapo OT, Ariba AJ, Odusoga OL. Changing patterns of emergency obstetric care at a Nigerian University hospital. Int J Gynaecol Obstet 2007;98:278–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
