

Lung microbiota across age and disease stage in cystic fibrosis
- PMID: 25974282
- PMCID: PMC4431465
- DOI: 10.1038/srep10241
Lung microbiota across age and disease stage in cystic fibrosis
Abstract
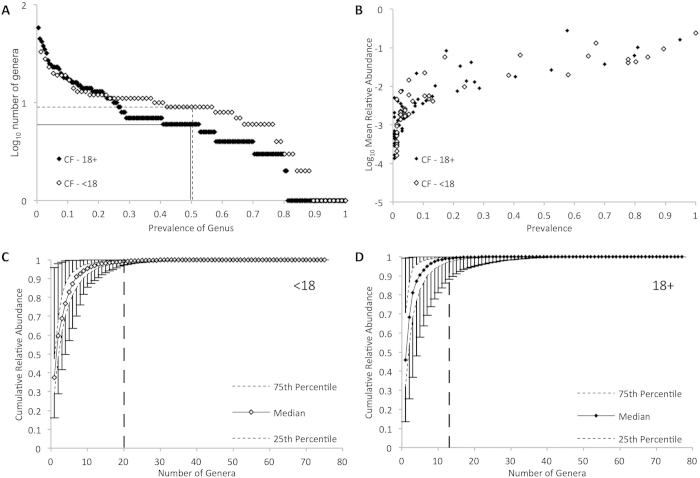
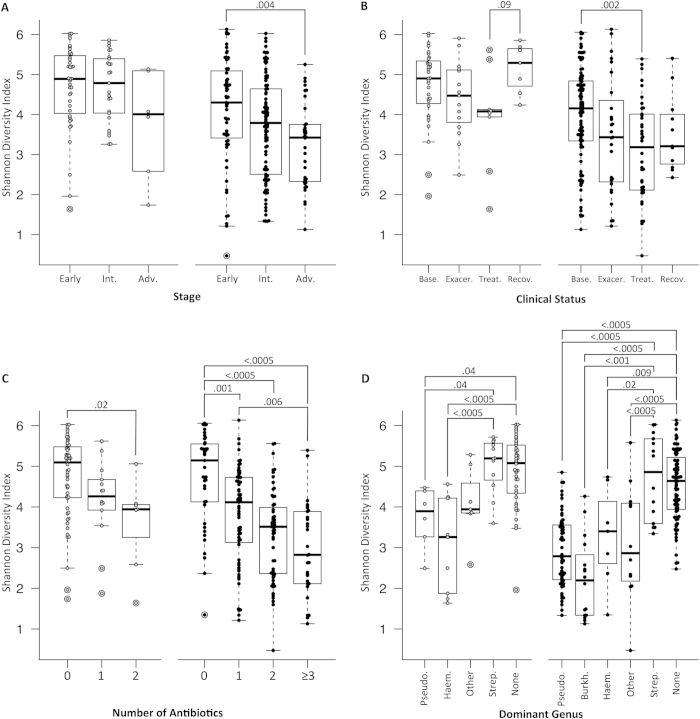
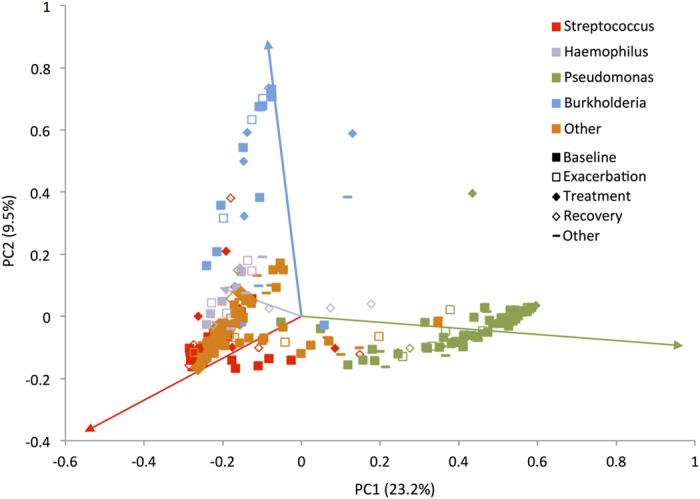
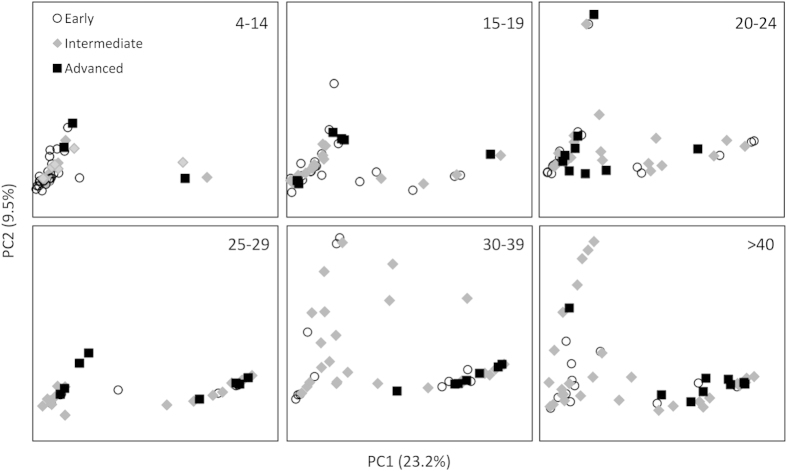
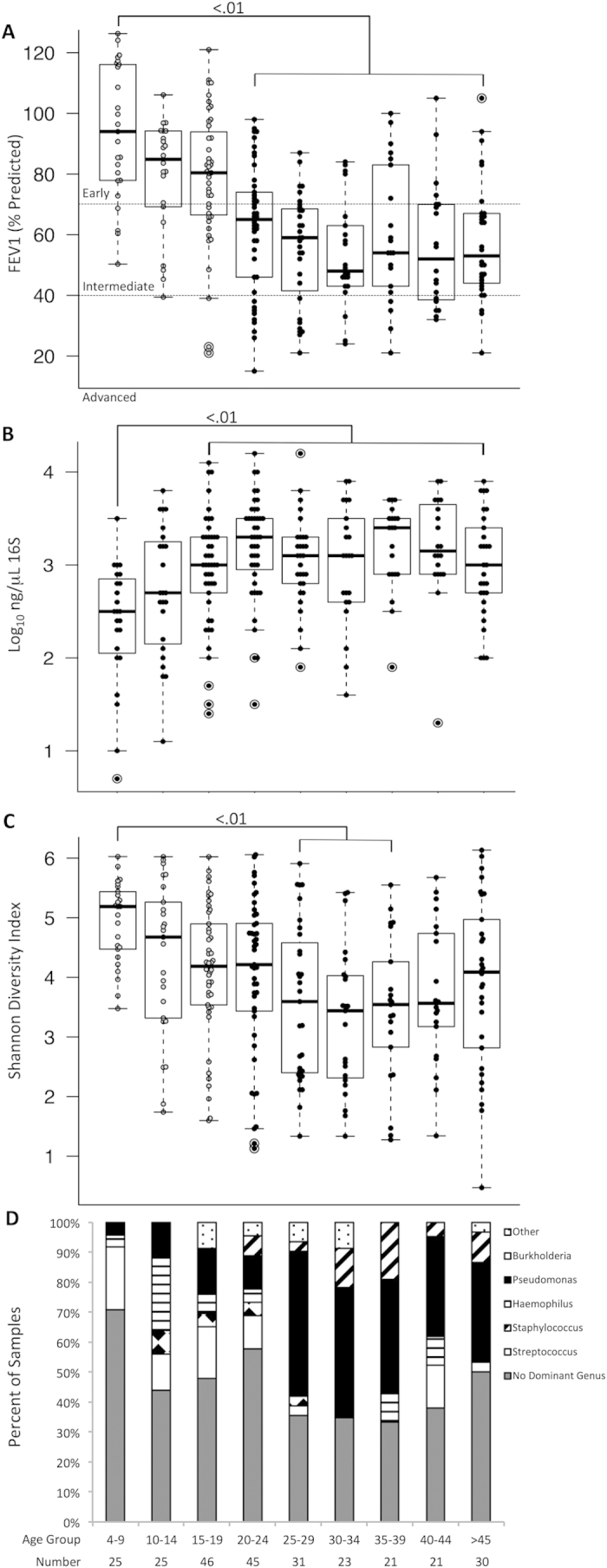
Understanding the significance of bacterial species that colonize and persist in cystic fibrosis (CF) airways requires a detailed examination of bacterial community structure across a broad range of age and disease stage. We used 16S ribosomal RNA sequencing to characterize the lung microbiota in 269 CF patients spanning a 60 year age range, including 76 pediatric samples from patients of age 4-17, and a broad cross-section of disease status to identify features of bacterial community structure and their relationship to disease stage and age. The CF lung microbiota shows significant inter-individual variability in community structure, composition and diversity. The core microbiota consists of five genera - Streptococcus, Prevotella, Rothia, Veillonella and Actinomyces. CF-associated pathogens such as Pseudomonas, Burkholderia, Stenotrophomonas and Achromobacter are less prevalent than core genera, but have a strong tendency to dominate the bacterial community when present. Community diversity and lung function are greatest in patients less than 10 years of age and lower in older age groups, plateauing at approximately age 25. Lower community diversity correlates with worse lung function in a multivariate regression model. Infection by Pseudomonas correlates with age-associated trends in community diversity and lung function.
Figures
References
-
- Kosorok M. R. et al. Acceleration of lung disease in children with cystic fibrosis after Pseudomonas aeruginosa acquisition. Pediatr Pulmonol 32, 277–287 (2001). - PubMed
-
- Huang N. N. et al. Clinical features, survival rate, and prognostic factors in young adults with cystic fibrosis. Am. J. Med 82, 871–879 (1987). - PubMed
-
- Lewin L. O., Byard P. J. & Davis P. B. Effect of Pseudomonas cepacia colonization on survival and pulmonary function of cystic fibrosis patients. J. Clin Epidemiol 43, 125–131 (1990). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
