

Antibiotics, pediatric dysbiosis, and disease
- PMID: 25974298
- PMCID: PMC5555213
- DOI: 10.1016/j.chom.2015.04.006
Antibiotics, pediatric dysbiosis, and disease
Abstract
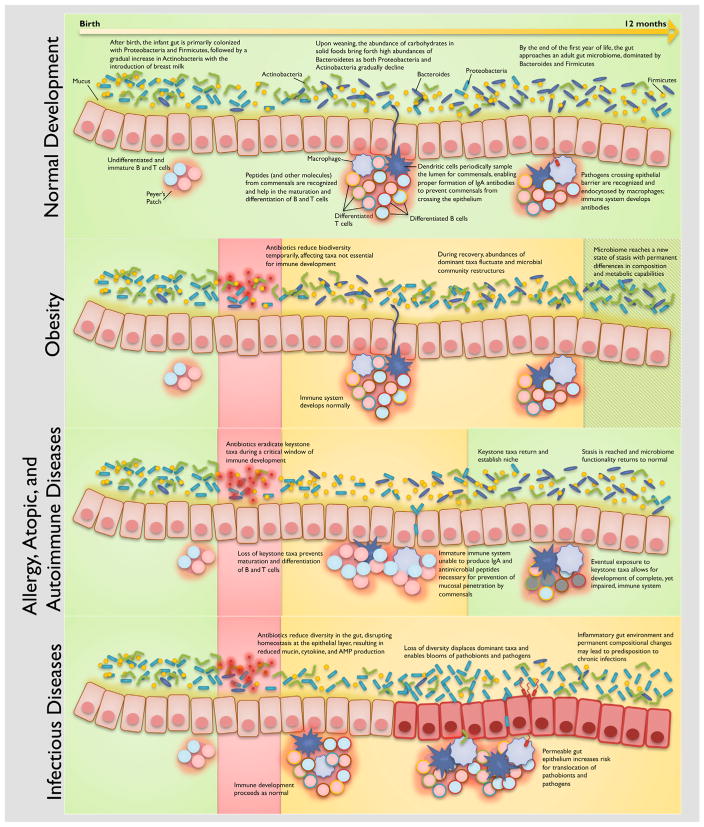
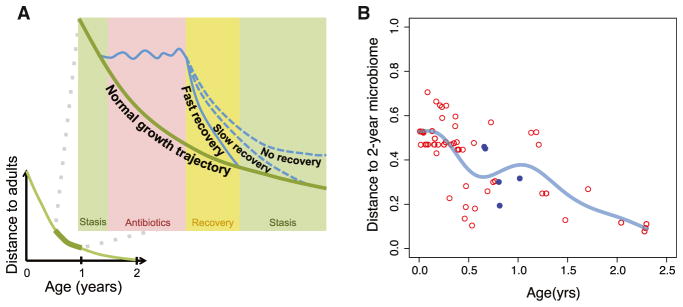
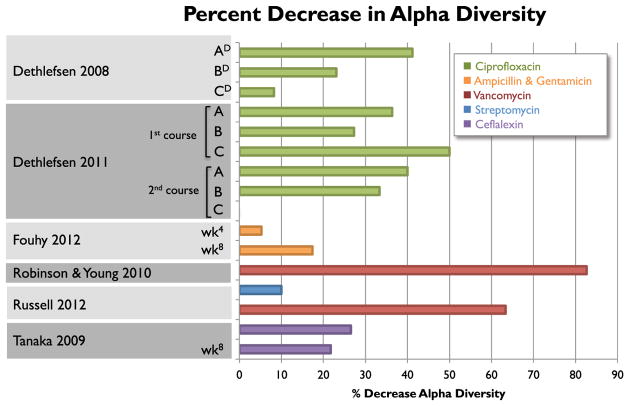
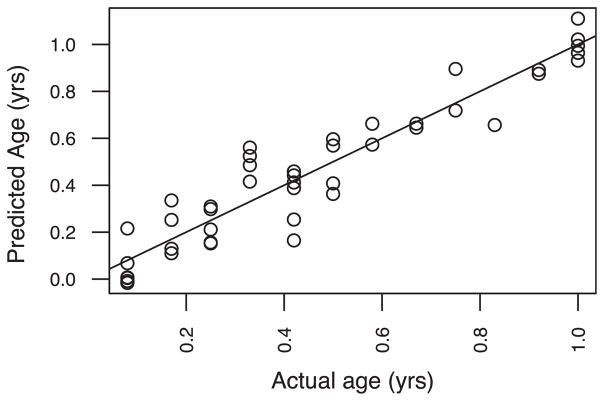
Antibiotics are by far the most common medications prescribed for children. Recent epidemiological data suggests an association between early antibiotic use and disease phenotypes in adulthood. Antibiotic use during infancy induces imbalances in gut microbiota, called dysbiosis. The gut microbiome's responses to antibiotics and its potential link to disease development are especially complex to study in the changing infant gut. Here, we synthesize current knowledge linking antibiotics, dysbiosis, and disease and propose a framework for studying antibiotic-related dysbiosis in children. We recommend future studies into the microbiome-mediated effects of antibiotics focused on four types of dysbiosis: loss of keystone taxa, loss of diversity, shifts in metabolic capacity, and blooms of pathogens. Establishment of a large and diverse baseline cohort to define healthy infant microbiome development is essential to advancing diagnosis, interpretation, and eventual treatment of pediatric dysbiosis. This approach will also help provide evidence-based recommendations for antibiotic usage in infancy.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
References
-
- Aagaard K, Ma J, Antony KM, Ganu R, Petrosino J, Versalovic J. The placenta harbors a unique microbiome. Sci Transl Med. 2014;6 http://dx.doi.org/10.1126/scitranslmed.3008599. - DOI - PMC - PubMed
-
- Abrahamsson TR, Jakobsson HE, Andersson AF, Björkstén B, Engstrand L, Jenmalm MC. Low diversity of the gut microbiota in infants with atopic eczema. J Allergy Clin Immunol. 2012;129:434–440. - PubMed
-
- Adams RJ, Heazlewood SP, Gilshenan KS, O’Brien M, McGuckin MA, Florin THJ. IgG antibodies against common gut bacteria are more diagnostic for Crohn’s disease than IgG against mannan or flagellin. Am J Gastroenterol. 2008;103:386–396. - PubMed
-
- Adkins B, Leclerc C, Marshall-Clarke S. Neonatal adaptive immunity comes of age. Nat Rev Immunol. 2004;4:553–564. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
