

Wideband arrhythmia-Insensitive-rapid (AIR) pulse sequence for cardiac T1 mapping without image artifacts induced by an implantable-cardioverter-defibrillator
- PMID: 25975192
- PMCID: PMC4515197
- DOI: 10.1002/mrm.25712
Wideband arrhythmia-Insensitive-rapid (AIR) pulse sequence for cardiac T1 mapping without image artifacts induced by an implantable-cardioverter-defibrillator
Abstract
Purpose: To develop and evaluate a wideband arrhythmia-insensitive-rapid (AIR) pulse sequence for cardiac T1 mapping without image artifacts induced by implantable-cardioverter-defibrillator (ICD).
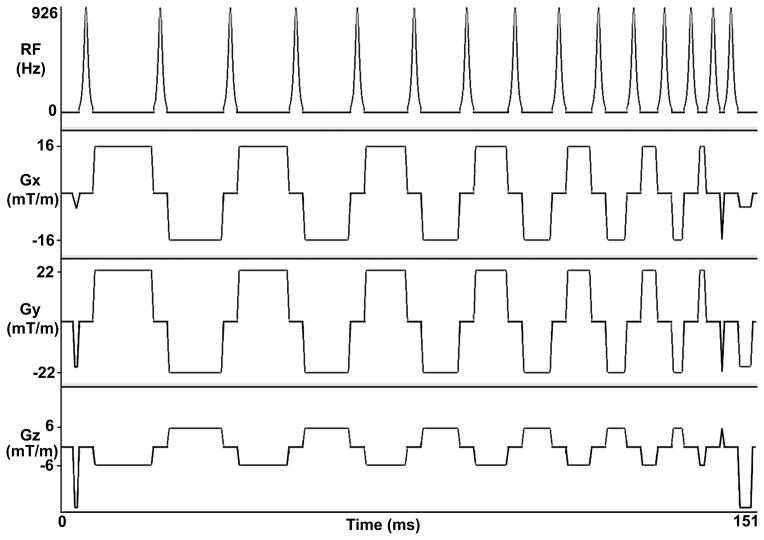
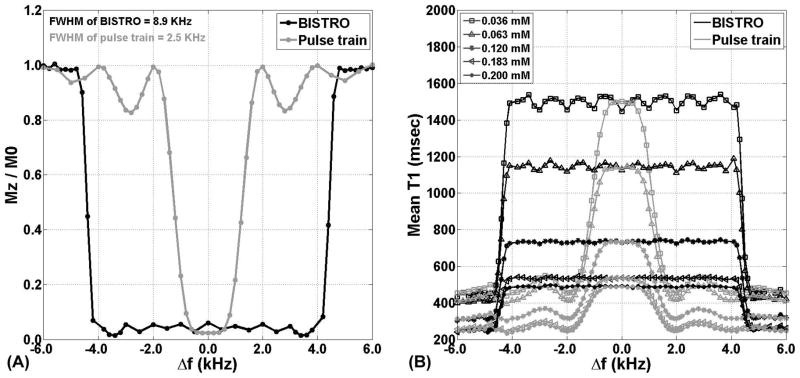
Methods: We developed a wideband AIR pulse sequence by incorporating a saturation pulse with wide frequency bandwidth (8.9 kHz) to achieve uniform T1 weighting in the heart with ICD. We tested the performance of original and "wideband" AIR cardiac T1 mapping pulse sequences in phantom and human experiments at 1.5 Tesla.
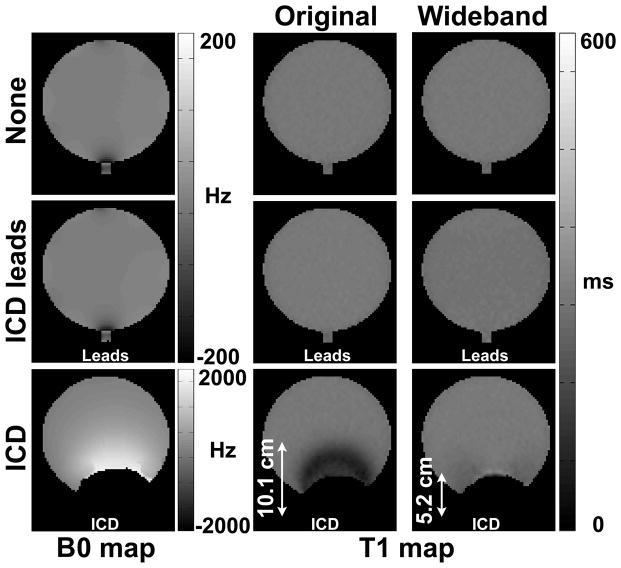
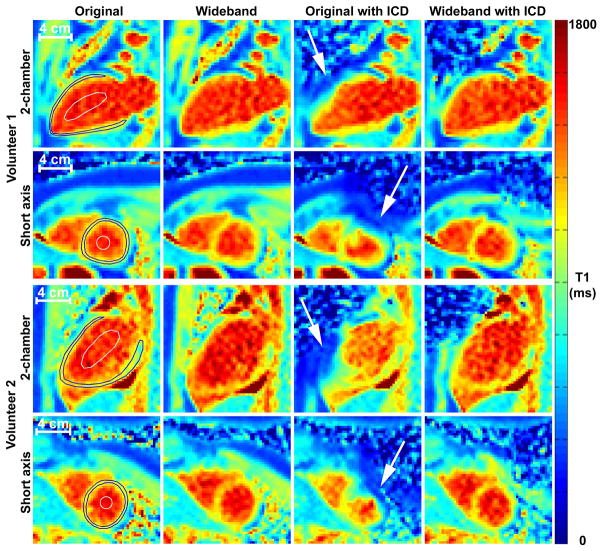
Results: In five phantoms representing native myocardium and blood and postcontrast blood/tissue T1 values, compared with the control T1 values measured with an inversion-recovery pulse sequence without ICD, T1 values measured with original AIR with ICD were considerably lower (absolute percent error > 29%), whereas T1 values measured with wideband AIR with ICD were similar (absolute percent error < 5%). Similarly, in 11 human subjects, compared with the control T1 values measured with original AIR without ICD, T1 measured with original AIR with ICD was significantly lower (absolute percent error > 10.1%), whereas T1 measured with wideband AIR with ICD was similar (absolute percent error < 2.0%).
Conclusion: This study demonstrates the feasibility of a wideband pulse sequence for cardiac T1 mapping without significant image artifacts induced by ICD.
Keywords: ECV; ICD; cardiac T1 mapping; heart failure; myocardial fibrosis; sudden cardiac death; wideband.
© 2015 Wiley Periodicals, Inc.
Figures

References
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. Heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation. 2013;127(1):e6–e245. - PMC - PubMed
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Drazner MH, Fonarow GC, Geraci SA, Horwich T, Januzzi JL, Johnson MR, Kasper EK, Levy WC, Masoudi FA, McBride PE, McMurray JJV, Mitchell JE, Peterson PN, Riegel B, Sam F, Stevenson LW, Tang WHW, Tsai EJ, Wilkoff BL. 2013 ACCF/AHA Guideline for the Management of Heart FailureA Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology. 2013;62(16):e147–e239. - PubMed
-
- Simmons A, Tofts PS, Barker GJ, Arridge SR. Sources of intensity nonuniformity in spin echo images at 1.5 T. Magn Reson Med. 1994;32(1):121–8. - PubMed
-
- Greenman RL, Shirosky JE, Mulkern RV, Rofsky NM. Double inversion black-blood fast spin-echo imaging of the human heart: a comparison between 1.5T and 3.0T. J Magn Reson Imaging. 2003;17(6):648–55. - PubMed
-
- Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW. 2009 Focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines Developed in Collaboration With the International Society for Heart and Lung Transplantation. J Am Coll Cardiol. 2009;53(15):e1–e90. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
