

Microanatomy of the cervical and anorectal squamocolumnar junctions: a proposed model for anatomical differences in HPV-related cancer risk
- PMID: 25975286
- PMCID: PMC4490106
- DOI: 10.1038/modpathol.2015.54
Microanatomy of the cervical and anorectal squamocolumnar junctions: a proposed model for anatomical differences in HPV-related cancer risk
Abstract
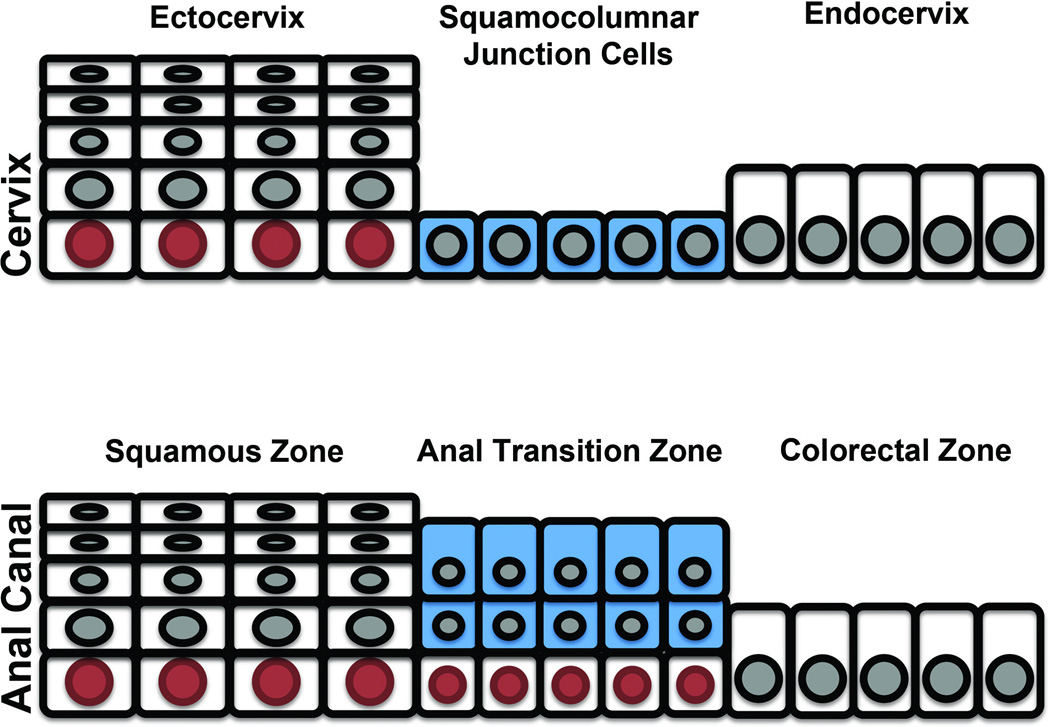
Human papilloma virus (HPV) infection causes cancers and their precursors (high-grade squamous intraepithelial lesions) near cervical and anal squamocolumnar junctions. Recently described cervical squamocolumnar junction cells are putative residual embryonic cells near the cervical transformation zone. These cells appear multipotential and share an identical immunophenotype (strongly CK7-positive) with over 90% of high-grade squamous intraepithelial lesions and cervical carcinomas. However, because the number of new cervical cancers discovered yearly world wide is 17-fold that of anal cancer, we posed the hypothesis that this difference in cancer risk reflects differences in the transition zones at the two sites. The microanatomy of the normal anal transformation zone (n=37) and topography and immunophenotype of anal squamous neoplasms (n=97) were studied. A discrete anal transition zone was composed of multilayered CK7-positive/p63-negative superficial columnar cells and an uninterrupted layer of CK7-negative/p63-positive basal cells. The CK7-negative/p63-positive basal cells were continuous with-and identical in appearance to-the basal cells of the mature squamous epithelium. This was in contrast to the cervical squamocolumnar junction, which harbored a single-layered CK7-positive/p63-negative squamocolumnar junction cell population. Of the 97 anal intraepithelial neoplasia/squamous cell carcinomas evaluated, only 27% (26/97) appeared to originate near the anal transition zone and only 23% (22/97) were CK7-positive. This study thus reveals two fundamental differences between the anus and the cervix: (1) the anal transition zone does not harbor a single monolayer of residual undifferentiated embryonic cells and (2) the dominant tumor immunophenotype is in keeping with an origin in metaplastic (CK7-negative) squamous rather than squamocolumnar junction (CK7-positive) epithelium. The implication is that, at birth, the embryonic cells in the anal transition zone have already begun to differentiate, presenting a metaplasia that-similar to vaginal and vulvar epithelium-is less prone to HPV-directed carcinogenesis. This in turn underscores the link between cancer risk and a very small and discrete population of vulnerable squamocolumnar junction cells in the cervix.
Figures


References
-
- Ferenczy A, Franco E. Persistent human papillomavirus infection and cervical neoplasia. Lancet Oncol. 2002;3:11–16. - PubMed
-
- Crum CP, Ikenberg H, Richart RM, Gissman L. Human papillomavirus type 16 and early cervical neoplasia. N Engl J Med. 1984;310:880–883. - PubMed
-
- Marsh M. Original site of cervical carcinoma; topographical relationship of carcinoma of the cervix to the external os and to the squamocolumnar junction. Obstet Gynecol. 1956;7:444–452. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
