

Subclassification of prostate cancer circulating tumor cells by nuclear size reveals very small nuclear circulating tumor cells in patients with visceral metastases
- PMID: 25975562
- PMCID: PMC4560974
- DOI: 10.1002/cncr.29455
Subclassification of prostate cancer circulating tumor cells by nuclear size reveals very small nuclear circulating tumor cells in patients with visceral metastases
Abstract
Background: Although enumeration of circulating tumor cells (CTCs) has shown some clinical value, the pool of CTCs contains a mixture of cells that contains additional information that can be extracted. The authors subclassified CTCs by shape features focusing on nuclear size and related this with clinical information.
Methods: A total of 148 blood samples were obtained from 57 patients with prostate cancer across the spectrum of metastatic states: no metastasis, nonvisceral metastasis, and visceral metastasis. CTCs captured and enumerated on NanoVelcro Chips (CytoLumina, Los Angeles, Calif) were subjected to pathologic review including nuclear size. The distribution of nuclear size was analyzed using a Gaussian mixture model. Correlations were made between CTC subpopulations and metastatic status.
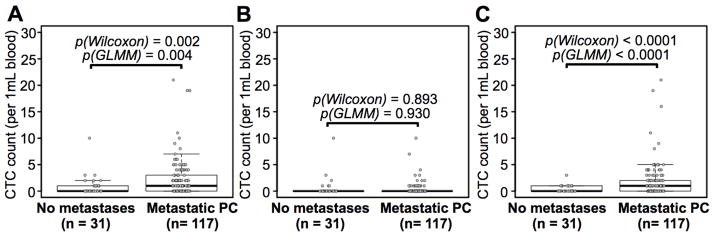
Results: Statistical modeling of nuclear size distribution revealed 3 distinct subpopulations: large nuclear CTCs, small nuclear CTCs, and very small nuclear CTCs (vsnCTCs). Small nuclear CTCs and vsnCTC identified those patients with metastatic disease. However, vsnCTC counts alone were found to be elevated in patients with visceral metastases when compared with those without (0.36 ± 0.69 vs 1.95 ± 3.77 cells/mL blood; P<.001). Serial enumeration studies suggested the emergence of vsnCTCs occurred before the detection of visceral metastases.
Conclusions: There are morphologic subsets of CTCs that can be identified by fundamental pathologic approaches, such as nuclear size measurement. The results of this observational study strongly suggest that CTCs contain relevant information regarding disease status. In particular, the detection of vsnCTCs was found to be correlated with the presence of visceral metastases and should be formally explored as a putative blood-borne biomarker to identify patients at risk of developing this clinical evolution of prostate cancer.
Keywords: NanoVelcro Chips; circulating tumor cells; nuclear size; prostate cancer; visceral metastasis.
© 2015 American Cancer Society.
Conflict of interest statement
Figures





Comment in
-
Circulating tumor cells in prostate cancer: Does (nuclear) size matter?Cancer. 2015 Sep 15;121(18):3190-2. doi: 10.1002/cncr.29454. Epub 2015 May 14. Cancer. 2015. PMID: 25980931 No abstract available.
References
-
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64:9–29. - PubMed
-
- Gandaglia G, Karakiewicz PI, Briganti A, et al. Impact of the Site of Metastases on Survival in Patients with Metastatic Prostate Cancer. Eur Urol. 2014 - PubMed
-
- Pond GR, Sonpavde G, de Wit R, Eisenberger MA, Tannock IF, Armstrong AJ. The prognostic importance of metastatic site in men with metastatic castration-resistant prostate cancer. Eur Urol. 2014;65:3–6. - PubMed
-
- Halabi S, Kelly WK, Zhou H, et al. The site of visceral metastases (mets) to predict overall survival (OS) in castration-resistant prostate cancer (CRPC) patients (pts): A meta-analysis of five phase III trials. J Clin Oncol. 2014;5s:2014. (suppl; abstr 5002)
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
