

Association of Predialysis Calculated Plasma Osmolarity With Intradialytic Blood Pressure Decline
- PMID: 25975966
- PMCID: PMC4782777
- DOI: 10.1053/j.ajkd.2015.03.028
Association of Predialysis Calculated Plasma Osmolarity With Intradialytic Blood Pressure Decline
Abstract
Background: The rapid reduction in plasma osmolality during hemodialysis (HD) may induce temporary gradients that promote the movement of water from the extracellular to the intracellular compartment, predisposing to the development of intradialytic hypotension (IDH).
Study design: Observational cohort study.
Setting & participants: 3,142 prevalent patients receiving thrice-weekly HD from a single dialysis provider organization.
Predictor: Predialysis calculated plasma osmolarity (calculated after the 2-day interval as 2 × serum sodium + serum urea nitrogen/2.8 + serum glucose/18).
Outcome: Magnitude of systolic blood pressure (SBP) decline (predialysis SBP - nadir intradialytic SBP) and risk of IDH (SBP decline > 35 or nadir SBP < 90 mm Hg).
Measurements: Unadjusted and multivariable-adjusted generalized linear models were fit to estimate the association of calculated osmolarity with intradialytic SBP decline and the odds of developing IDH.
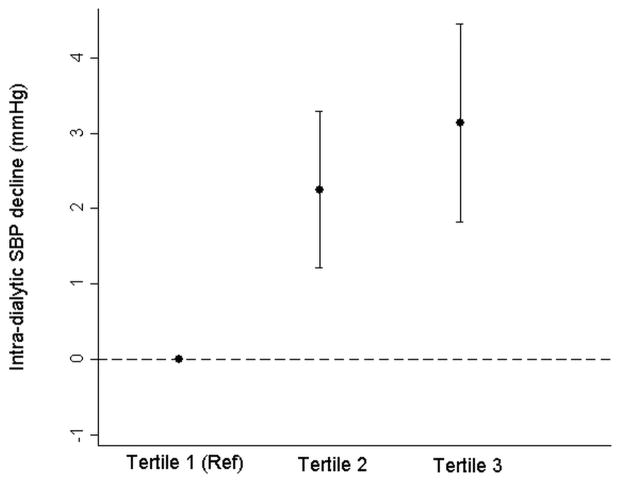
Results: Mean age of participants was 62.6±15.2 (SD) years, 57.1% were men, and 61.0% had diabetes. Mean predialysis calculated osmolarity during follow-up was 306.4 ± 9.5 mOsm/L. After case-mix adjustment, each 10-mOsm/L increase in predialysis calculated osmolarity was associated with 1.48 (95% CI, 0.86-2.09) mm Hg (P < 0.001) greater decline in intradialytic SBP and 10% greater odds of IDH (OR, 1.10; 95% CI, 1.05-1.15). In adjusted models, lower predialysis sodium and higher serum urea nitrogen and serum glucose levels were associated with greater decline in intradialytic SBP.
Limitations: Measured serum osmolality, timing of changes in intradialytic osmolality, dialysate osmolality, and dialysate temperature were not available.
Conclusions: Higher predialysis calculated osmolarity is associated with greater decline in intradialytic SBP and greater risk of IDH in maintenance HD patients. Strategies to minimize rapid shifts in osmolality should be tested prospectively to minimize excess SBP decline in susceptible patients.
Keywords: Intra-dialytic hypotension; calculated plasma osmolarity; end-stage renal disease (ESRD); hemodialysis; hemodynamic instability; osmolality; renal replacement therapy (RRT); systolic blood pressure (SBP).
Copyright © 2015 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Bos WJ, Bruin S, van Olden RW, et al. Cardiac and hemodynamic effects of hemodialysis and ultrafiltration. Am J Kidney Dis. 2000;35:819–826. - PubMed
-
- Boon D, van Montfrans GA, Koopman MG, Krediet RT, Bos WJ. Blood pressure response to uncomplicated hemodialysis: the importance of changes in stroke volume. Nephron Clin Pract. 2004;96:c82–87. - PubMed
-
- Palmer BF, Henrich WL. Recent advances in the prevention and management of intradialytic hypotension. J Am Soc Nephrol. 2008;19:8–11. - PubMed
-
- Owen PJ, Priestman WS, Sigrist MK, et al. Myocardial contractile function and intradialytic hypotension. Hemodial Int. 2009;13:293–300. - PubMed
-
- Mizumasa T, Hirakata H, Yoshimitsu T, et al. Dialysis-related hypotension as a cause of progressive frontal lobe atrophy in chronic hemodialysis patients: a 3-year prospective study. Nephron Clin Pract. 2004;97:c23–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
