

Utility of five commonly used immunohistochemical markers TTF-1, Napsin A, CK7, CK5/6 and P63 in primary and metastatic adenocarcinoma and squamous cell carcinoma of the lung: a retrospective study of 246 fine needle aspiration cases
- PMID: 25977750
- PMCID: PMC4417108
- DOI: 10.1186/s40169-015-0057-2
Utility of five commonly used immunohistochemical markers TTF-1, Napsin A, CK7, CK5/6 and P63 in primary and metastatic adenocarcinoma and squamous cell carcinoma of the lung: a retrospective study of 246 fine needle aspiration cases
Abstract
Background: Fine needle aspiration (FNA) biopsy plays a critical role in the diagnosis and staging of lung primary and metastatic lung carcinoma. Accurate subclassification of adenocarcinoma (ADC) and/or squamous cell carcinoma (SqCC) is crucial for the targeted therapy. However, the distinction between ADC and SqCC may be difficult in small FNA specimens. Here, we have retrospectively evaluated the utility of TTF-1, Napsin A, CK7, P63 and CK5/6 immunohistochemical (IHC) markers in the distinguishing and subclassification of ADC and SqCC.
Methods: A total of 246 FNA cases were identified by a computer search over a two-year period, including 102 primary NSCLC and 144 primary NSCLC which had metastasized to other sites. The immunostaining patterns of TTF-1, Napsin A, CK7, P63 and CK5/6 were correlated with the histological diagnosis of the tumor.
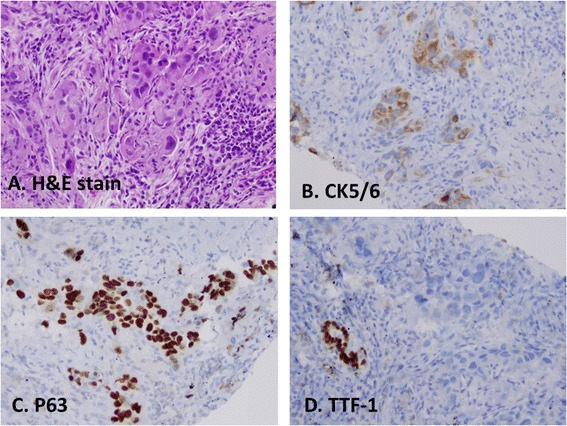
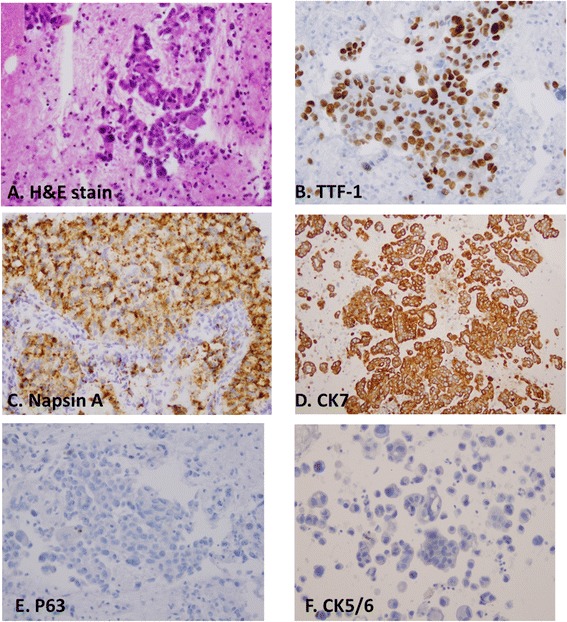
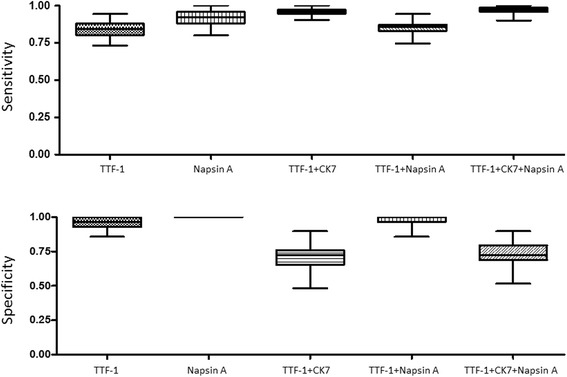
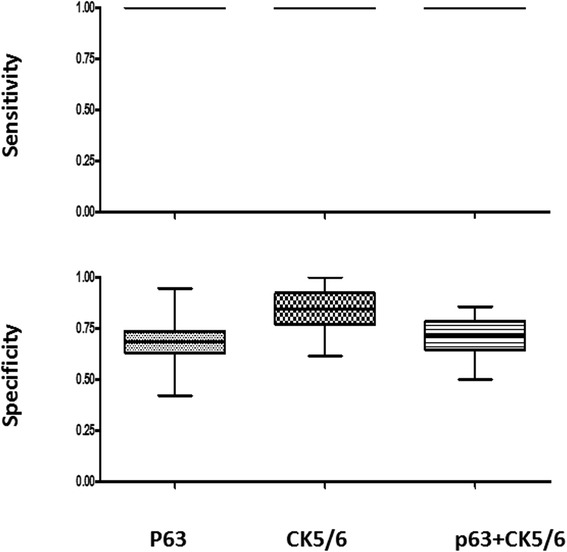
Results: In 72 primary ADCs, TTF-1, Napsin A and CK7 showed a sensitivity and specificity of 84.5%/96.4%, 92.0%/100%, and 93.8%/50.0%. In 30 primary SqCCs, CK5/6 and P63 showed a sensitivity and specificity of 100%/77.8% and 91.7%/78.3%. In 131 metastatic ADCs, Napsin A showed the highest specificity (100%), versus TTF-1 (87.5%) and CK7 (25%) but decreased sensitivity (67.8% versus 86.9% and 100%); whereas in 13 metastatic SqCCs, CK5/6 and P63 showed a sensitivity/specificity of 100%/84.6% and 100%/68.4%. Bootstrap analysis showed that the combination of TTF-1/CK7, TTF-1/Napsin A and TTF-1/CK7/Napsin A had a sensitivity/specificity of 0.960/0.732, 0.858/0.934, 0.972/0.733 for primary lung ADCs and 0.992/0.642, 0.878/0.881, 0.993/0.618 for metastatic lung ADCs.
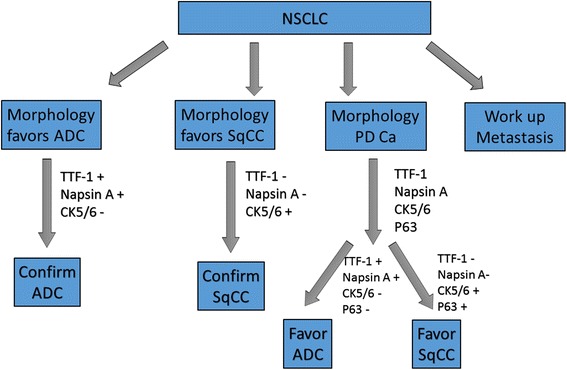
Conclusions: Our study demonstrated that IHC markers had variable sensitivity and specificity in the subclassification of primary and metastatic ADC and SqCC. Based on morphological findings, an algorithm with the combination use of markers aided in the subclassification of NSCLCs in difficult cases.
Keywords: CK7; Cytopathology; Fine needle aspiration (FNA) cytology; Immunohistochemical (IHC) marker; Napsin A; Non-small cell lung carcinoma (NSCLC); P63 and CK5/6; TTF-1.
Figures


References
-
- Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011;6:244–285. doi: 10.1097/JTO.0b013e318206a221. - DOI - PMC - PubMed
-
- Travis WD, World Health Organization., International Agency for Research on Cancer., International Academy of Pathology., International Association for the Study of Lung Cancer . Pathology and genetics of tumours of the lung, pleura, thymus and heart. Lyon ; Great Britain: IARC Press; 2004. p. 344.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials