

The influence of genetic variability and proinflammatory status on the development of bone disease in patients with Gaucher disease
- PMID: 25978039
- PMCID: PMC4433334
- DOI: 10.1371/journal.pone.0126153
The influence of genetic variability and proinflammatory status on the development of bone disease in patients with Gaucher disease
Abstract
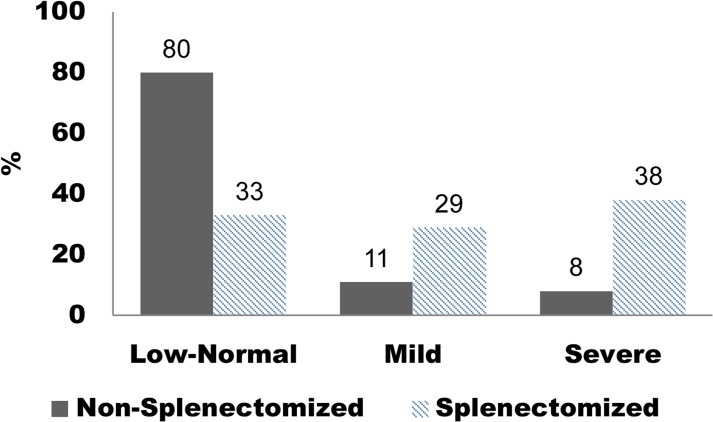
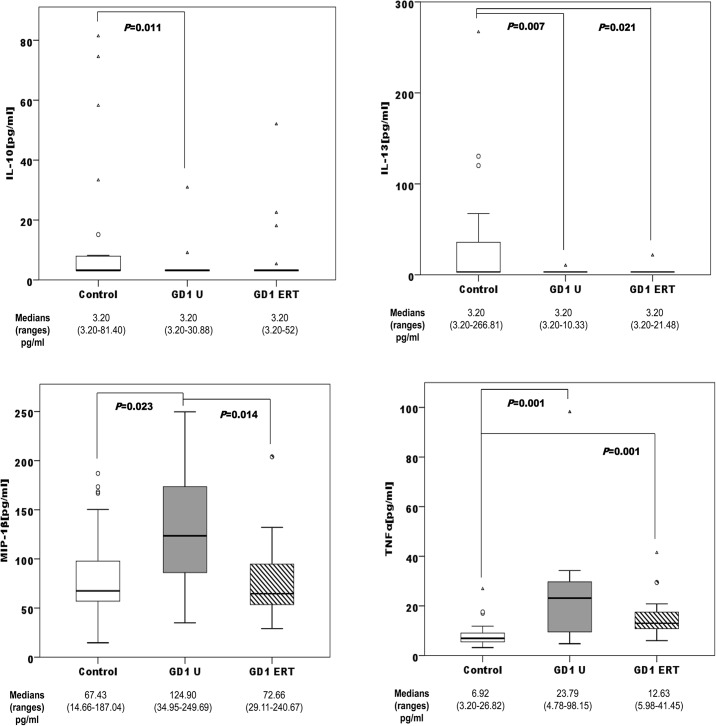
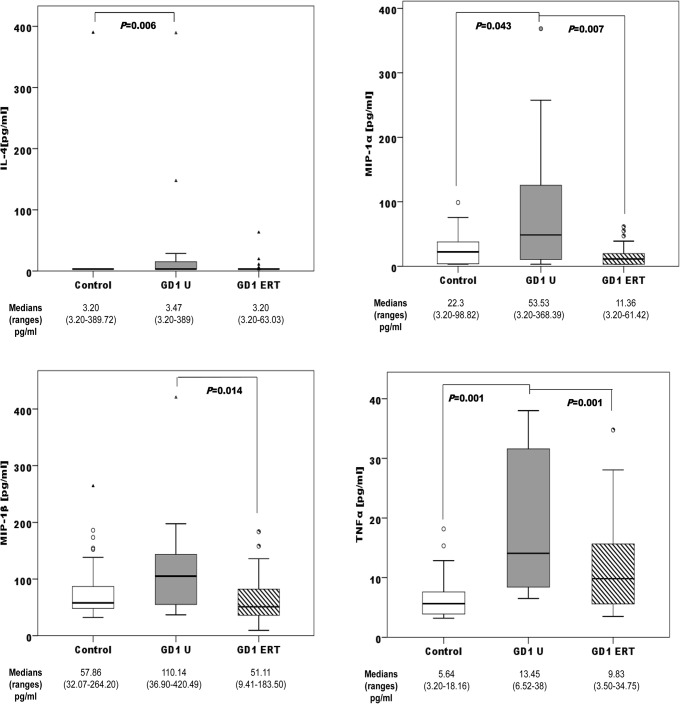
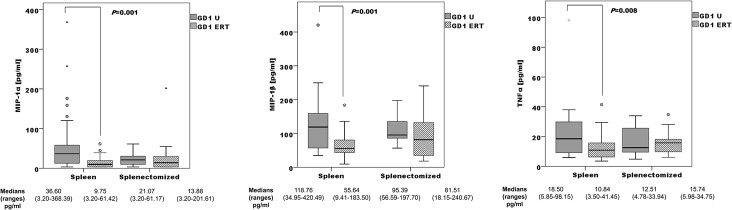
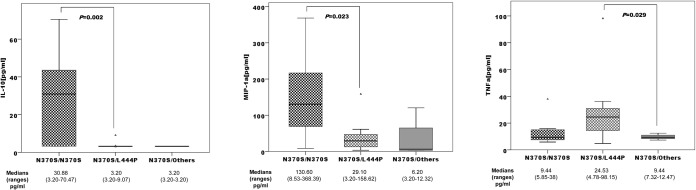
Gaucher disease, the most common lysosomal storage disorder, is caused by β-glucocerebrosidase deficiency. Bone complications are the major cause of morbidity in patients with type 1 Gaucher disease (GD1). Genetic components strongly influence bone remodelling. In addition, chronic inflammation produced by Gaucher cells induces the production of several cytokines, which leads to direct changes in the bone remodelling process and can also affect the process indirectly through other immune cells. In this study, we analysed the association between bone mineral density (BMD), bone marrow burden score, and relevant genetic polymorphisms related to bone metabolism, as well as profiles of proinflammatory cytokines in a GD1 cohort. This study included 83 patients distributed according to bone status. BMD was measured with DXA and broadband ultrasound attenuation; bone marrow involvement was evaluated using MRI. We also analysed 26 SNPs located in 14 genes related to bone metabolism. To assess proinflammatory status, we analysed IL-4, IL-6, IL-7, IL-10, IL-13, MIP-1α, MIP-1β, and TNFα in plasma samples from 71 control participants and GD1 patients. SNP genotype proportions and BMD differed significantly between ESRI c.453-397T>C and VDR c.1024+283G>A variants. We also observed significant associations between GD1 genotypes and bone affectation. When patients were stratified by spleen status, we observed significant correlations between non-/splenectomized groups and Spanish MRI (S-MRI) score. Across genotype proportions of non-/splenectomized patients and S-MRI, we observed significant differences in ESRI c.453-397T>C, VDR c.-83-25988G>A, and TNFRSF11B c.9C>G polymorphisms. We observed different significant proinflammatory profiles between control participants, treatment-naïve patients, and patients on enzyme replacement therapy (ERT); between non-/splenectomized patients (between untreated and ERT-treated patients) and among those with differing GBA genotypes. The data suggest that patients with GD1 have increased susceptibility to developing bone disease owing to the coexistence of genetic variants, and that genetic background in GD1 is fundamental to regulate the impact of proinflammatory status on the development of bone disease.
Conflict of interest statement
Figures
Similar articles
-
Gene variants of osteoprotegerin, estrogen-, calcitonin- and vitamin D-receptor genes and serum markers of bone metabolism in patients with Gaucher disease type 1.Ther Clin Risk Manag. 2018 Oct 24;14:2069-2080. doi: 10.2147/TCRM.S177480. eCollection 2018. Ther Clin Risk Manag. 2018. PMID: 30498352 Free PMC article.
-
Risk factors for fractures and avascular osteonecrosis in type 1 Gaucher disease: a study from the International Collaborative Gaucher Group (ICGG) Gaucher Registry.J Bone Miner Res. 2012 Aug;27(8):1839-48. doi: 10.1002/jbmr.1680. J Bone Miner Res. 2012. PMID: 22692814
-
Ferritinemia and serum inflammatory cytokines in Swedish adults with Gaucher disease type 1.Blood Cells Mol Dis. 2018 Feb;68:35-42. doi: 10.1016/j.bcmd.2016.10.010. Epub 2016 Oct 20. Blood Cells Mol Dis. 2018. PMID: 27816428
-
Bone complications in children with Gaucher disease.Br J Radiol. 2002;75 Suppl 1:A37-44. doi: 10.1259/bjr.75.suppl_1.750037. Br J Radiol. 2002. PMID: 12036831 Review.
-
Response of Gaucher bone disease to enzyme replacement therapy.Br J Radiol. 2002;75 Suppl 1:A25-36. doi: 10.1259/bjr.75.suppl_1.750025. Br J Radiol. 2002. PMID: 12036830 Review.
Cited by
-
Old disease-New reflections: Gaucher, immunity, and inflammation.J Cell Mol Med. 2024 Oct;28(20):e70087. doi: 10.1111/jcmm.70087. J Cell Mol Med. 2024. PMID: 39463025 Free PMC article. Review.
-
An increase in ER stress and unfolded protein response in iPSCs-derived neuronal cells from neuronopathic Gaucher disease patients.Sci Rep. 2024 Apr 22;14(1):9177. doi: 10.1038/s41598-024-59834-6. Sci Rep. 2024. PMID: 38649404 Free PMC article.
-
Identification of risk features for complication in Gaucher's disease patients: a machine learning analysis of the Spanish registry of Gaucher disease.Orphanet J Rare Dis. 2020 Sep 22;15(1):256. doi: 10.1186/s13023-020-01520-7. Orphanet J Rare Dis. 2020. PMID: 32962737 Free PMC article.
-
Expression Profiles of Exosomal miRNAs in Gaucher Patients and Their Association With Severity of Bone Involvement.J Inherit Metab Dis. 2025 Jul;48(4):e70061. doi: 10.1002/jimd.70061. J Inherit Metab Dis. 2025. PMID: 40619747 Free PMC article.
-
Reconstruction of the Cytokine Signaling in Lysosomal Storage Diseases by Literature Mining and Network Analysis.Front Cell Dev Biol. 2021 Aug 20;9:703489. doi: 10.3389/fcell.2021.703489. eCollection 2021. Front Cell Dev Biol. 2021. PMID: 34490253 Free PMC article.
References
-
- Beutler E, Grabowski G. Gaucher Disease In: Scriber C, Beudet A, Sly W, Valle D, editors. The metabolic basis of inherited disease. New York: McGraw Hill; 2001. p. 3635–68.
-
- Giraldo P, Pocovi M, Perez-Calvo J, Rubio-Felix D, Giralt M. Report of the Spanish Gaucher's disease registry: clinical and genetic characteristics. Haematologica. 2000;85(8):792–9. - PubMed
-
- Wenstrup RJ, Roca-Espiau M, Weinreb NJ, Bembi B. Skeletal aspects of Gaucher disease: a review. Br J Radiol. 2002;75 Suppl 1:A2–12. - PubMed
-
- Eriksen E, Axelrod D, Melsen F. Bone histology and bone histomorphometry In: Eriksen E, Axelrod D, Melsen F, editors. Bone Histomorphometry. New York: Raven Press; 1994. p. 33–48.
-
- Nguyen TV, Blangero J, Eisman JA. Genetic epidemiological approaches to the search for osteoporosis genes. J Bone Miner Res. 2000;15(3):392–401. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
