

Global Association of Cold Spells and Adverse Health Effects: A Systematic Review and Meta-Analysis
- PMID: 25978526
- PMCID: PMC4710591
- DOI: 10.1289/ehp.1408104
Global Association of Cold Spells and Adverse Health Effects: A Systematic Review and Meta-Analysis
Abstract
Background: There is substantial evidence that mortality increases in low temperatures. Less is known about the role of prolonged cold periods denoted as cold spells.
Objective: We conducted the first systematic review and meta-analysis to summarize the evidence on the adverse health effects of cold spells in varying climates.
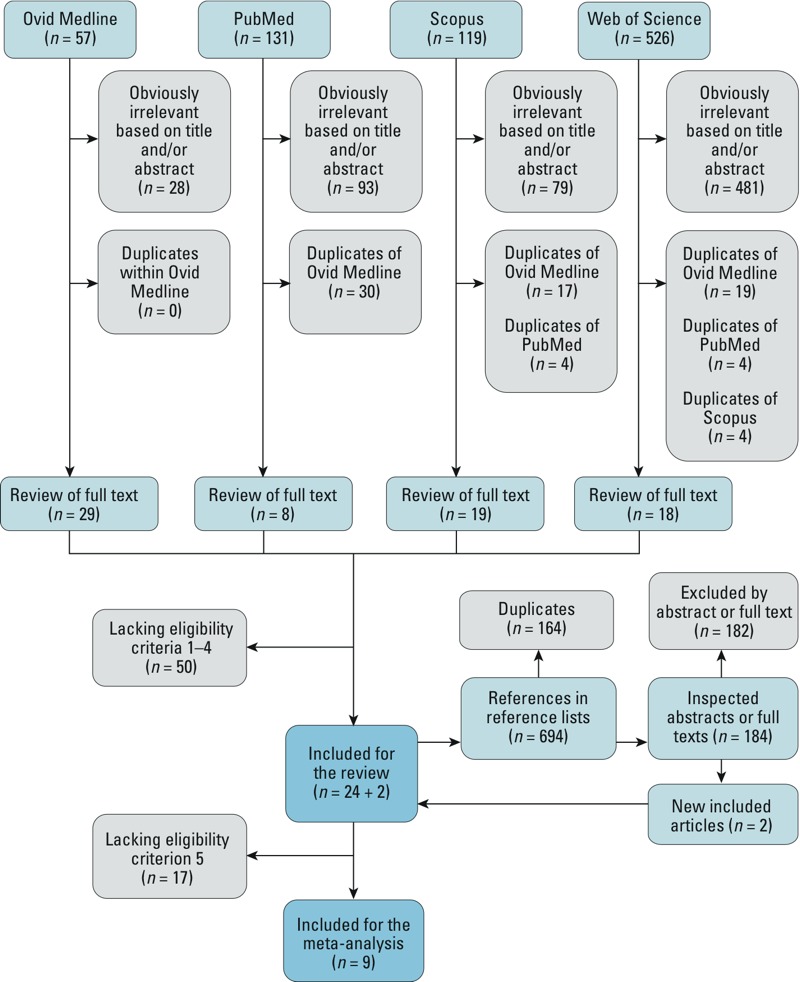
Data sources and extraction: Four databases (Ovid Medline, PubMed, Scopus, Web of Science) were searched for all years and languages available. "Cold spell" was defined as an event below a temperature threshold lasting for a minimum duration of 2 days. Of 1,527 identified articles, 26 satisfied our eligibility criteria for the systematic review, and 9 were eligible for meta-analyses. The articles were grouped by the three main study questions into Overall-effect Group, Added-effect Group, and Temperature-change-effect Group.
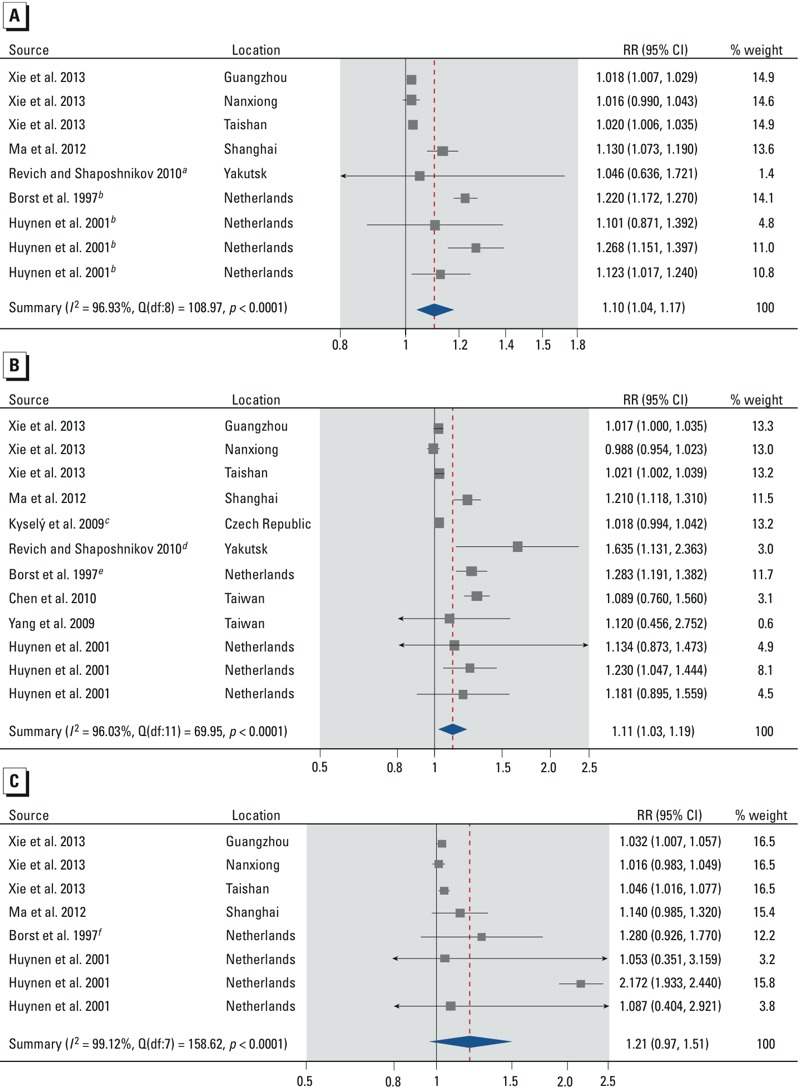
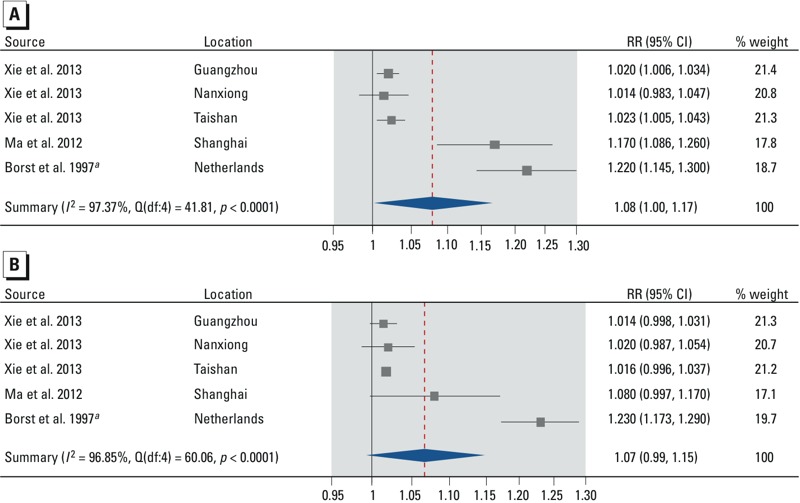
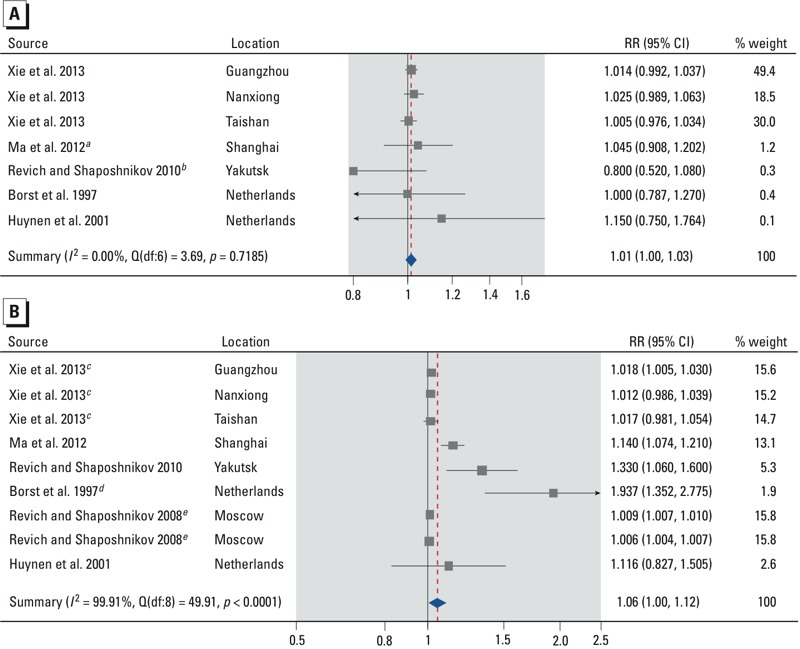
Data synthesis: Based on random-effects models in the meta-analyses, cold spells were associated with increased mortality from all or all nonaccidental causes (summary rate ratio = 1.10; 95% CI: 1.04, 1.17 based on 9 estimates from five studies), cardiovascular diseases (1.11; 95% CI: 1.03, 1.19; 12 estimates from eight studies), and respiratory diseases (1.21; 95% CI: 0.97, 1.51; 8 estimates from four studies). Estimated associations were stronger for people ≥ 65 years of age (1.06; 95% CI: 1.00, 1.12) than for people 0-64 years of age (1.01; 95% CI: 1.00, 1.03). Study-specific effect estimates from a limited number of studies suggested an increased morbidity related to cold spells, but it was not possible to quantitatively summarize the evidence.
Conclusions: Cold spells are associated with increased mortality rates in populations around the world. The body of evidence suggests that cold spells also have other adverse health effects. There was substantial heterogeneity among the studies, which should be taken into account in the interpretation of the results.
Citation: Ryti NR, Guo Y, Jaakkola JJ. 2016. Global association of cold spells and adverse health effects: a systematic review and meta-analysis. Environ Health Perspect 124:12-22; http://dx.doi.org/10.1289/ehp.1408104.
Conflict of interest statement
The authors declare they have no actual or potential competing financial interests.
Figures
References
-
- Analitis A, Katsouyanni K, Biggeri A, Baccini M, Forsberg B, Bisanti L, et al. Effects of cold weather on mortality: results from 15 European cities within the PHEWE project. Am J Epidemiol. 2008;168:1397–1408. - PubMed
-
- Barnett AG, Hajat S, Gasparrini A, Rocklöv J. Cold and heat waves in the United States. Environ Res. 2012;112:218–224. - PubMed
-
- Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. In: Introduction to Meta-Analysis. Chichester, West Sussex, United Kingdom: John Wiley & Sons Ltd; 2009. Identifying and quantifying heterogeneity; pp. 107–125.
-
- Borst V, Schols JMGA, Mackenbach JP. Increased mortality among nursing home patients during ambient temperature extremes; more rise during hot than during cold spells [in Dutch]. Ned Tijdschr Geneeskd. 1997;141:2180–2183.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
