

Physiology of breathlessness associated with pleural effusions
- PMID: 25978627
- PMCID: PMC5633324
- DOI: 10.1097/MCP.0000000000000174
Physiology of breathlessness associated with pleural effusions
Abstract
Purpose of review: Pleural effusions have a major impact on the cardiorespiratory system. This article reviews the pathophysiological effects of pleural effusions and pleural drainage, their relationship with breathlessness, and highlights key knowledge gaps.
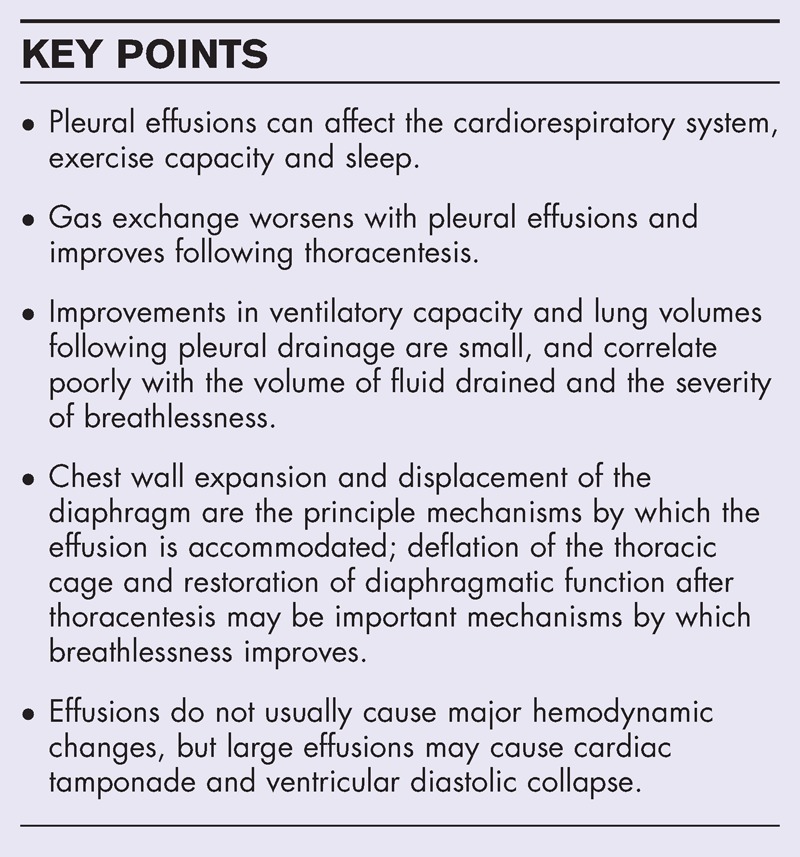
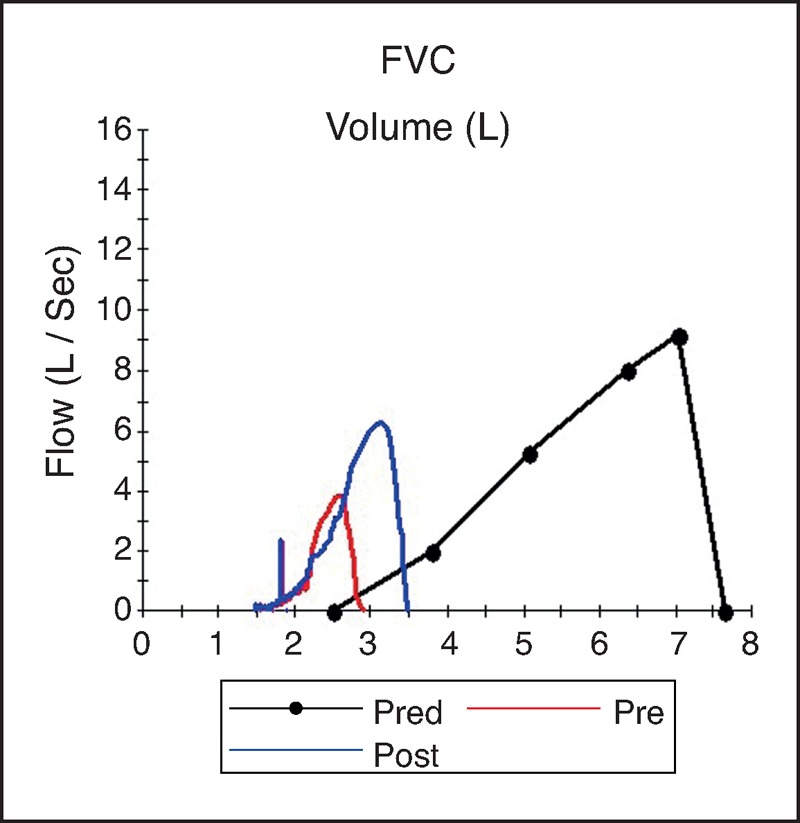
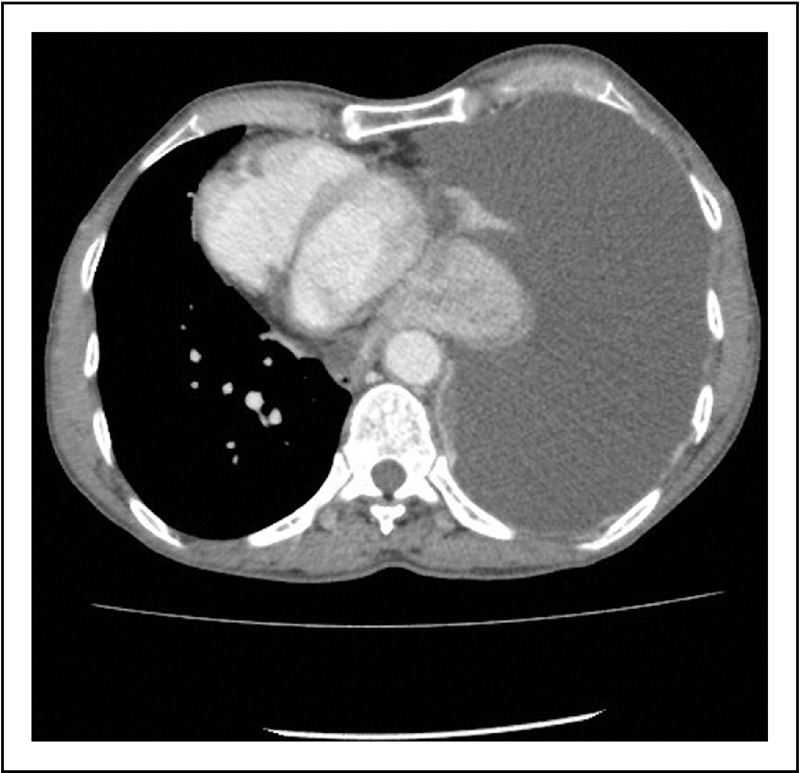
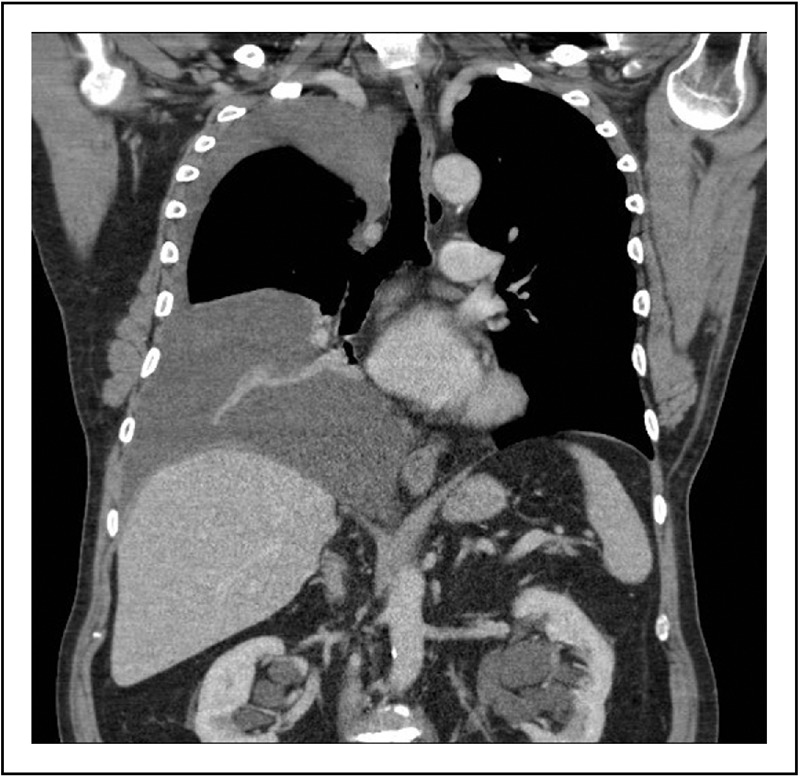
Recent findings: The basis for breathlessness in pleural effusions and relief following thoracentesis is not well understood. Many existing studies on the pathophysiology of breathlessness in pleural effusions are limited by small sample sizes, heterogeneous design and a lack of direct measurements of respiratory muscle function. Gas exchange worsens with pleural effusions and improves after thoracentesis. Improvements in ventilatory capacity and lung volumes following pleural drainage are small, and correlate poorly with the volume of fluid drained and the severity of breathlessness. Rather than lung compression, expansion of the chest wall, including displacement of the diaphragm, appears to be the principle mechanism by which the effusion is accommodated. Deflation of the thoracic cage and restoration of diaphragmatic function after thoracentesis may improve diaphragm effectiveness and efficiency, and this may be an important mechanism by which breathlessness improves. Effusions do not usually lead to major hemodynamic changes, but large effusions may cause cardiac tamponade and ventricular diastolic collapse. Patients with effusions can have impaired exercise capacity and poor sleep quality and efficiency.
Summary: Pleural effusions are associated with abnormalities in gas exchange, respiratory mechanics, respiratory muscle function and hemodynamics, but the association between these abnormalities and breathlessness remains unclear. Prospective studies should aim to identify the key mechanisms of effusion-related breathlessness and predictors of improvement following pleural drainage.
Figures
References
-
- Light RW. Pleural diseases. 4th ed.Philadelphia:Lippincott Williams & Wilkins; 2001. 89.
-
- Marel M, Zrustova M, Stasny B, et al. The incidence of pleural effusion in a well defined region. Epidemiologic study in central Bohemia. Chest 1993; 104:1486–1489. - PubMed
-
- Cartaxo AM, Vargas FS, Salge JM, et al. Improvements in the 6-min walk test and spirometry following thoracentesis for symptomatic pleural effusions. Chest 2011; 139:1424–1429. - PubMed
-
This prospective study of 25 patients is the only one to assess the effect of pleural effusions on exercise capacity, and showed that thoracentesis significantly improves breathlessness and the 6-min walk distance.
-
- Estenne M, Yernault JC, De Troyer A. Mechanism of relief of dyspnea after thoracocentesis in patients with large pleural effusions. Am J Med 1983; 74:813–819. - PubMed
-
- Wang JS, Tseng CH. Changes in pulmonary mechanics and gas exchange after thoracentesis on patients with inversion of a hemidiaphragm secondary to large pleural effusion. Chest 1995; 107:1610–1614. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
