

Motion mitigation for lung cancer patients treated with active scanning proton therapy
- PMID: 25979039
- PMCID: PMC4409624
- DOI: 10.1118/1.4916662
Motion mitigation for lung cancer patients treated with active scanning proton therapy
Abstract
Purpose: Motion interplay can affect the tumor dose in scanned proton beam therapy. This study assesses the ability of rescanning and gating to mitigate interplay effects during lung treatments.
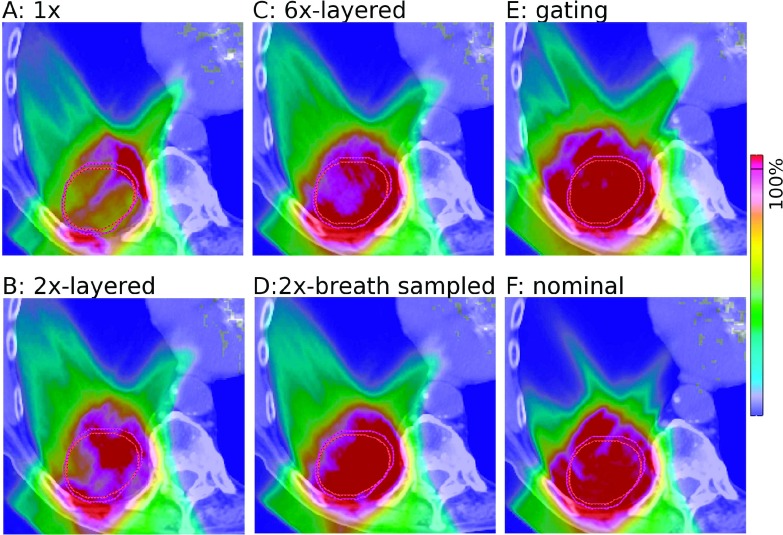
Methods: The treatments of five lung cancer patients [48 Gy(RBE)/4fx] with varying tumor size (21.1-82.3 cm(3)) and motion amplitude (2.9-30.6 mm) were simulated employing 4D Monte Carlo. The authors investigated two spot sizes (σ ∼ 12 and ∼ 3 mm), three rescanning techniques (layered, volumetric, breath-sampled volumetric) and respiratory gating with a 30% duty cycle.
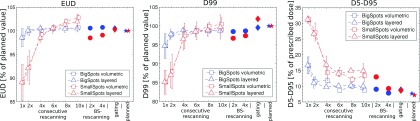
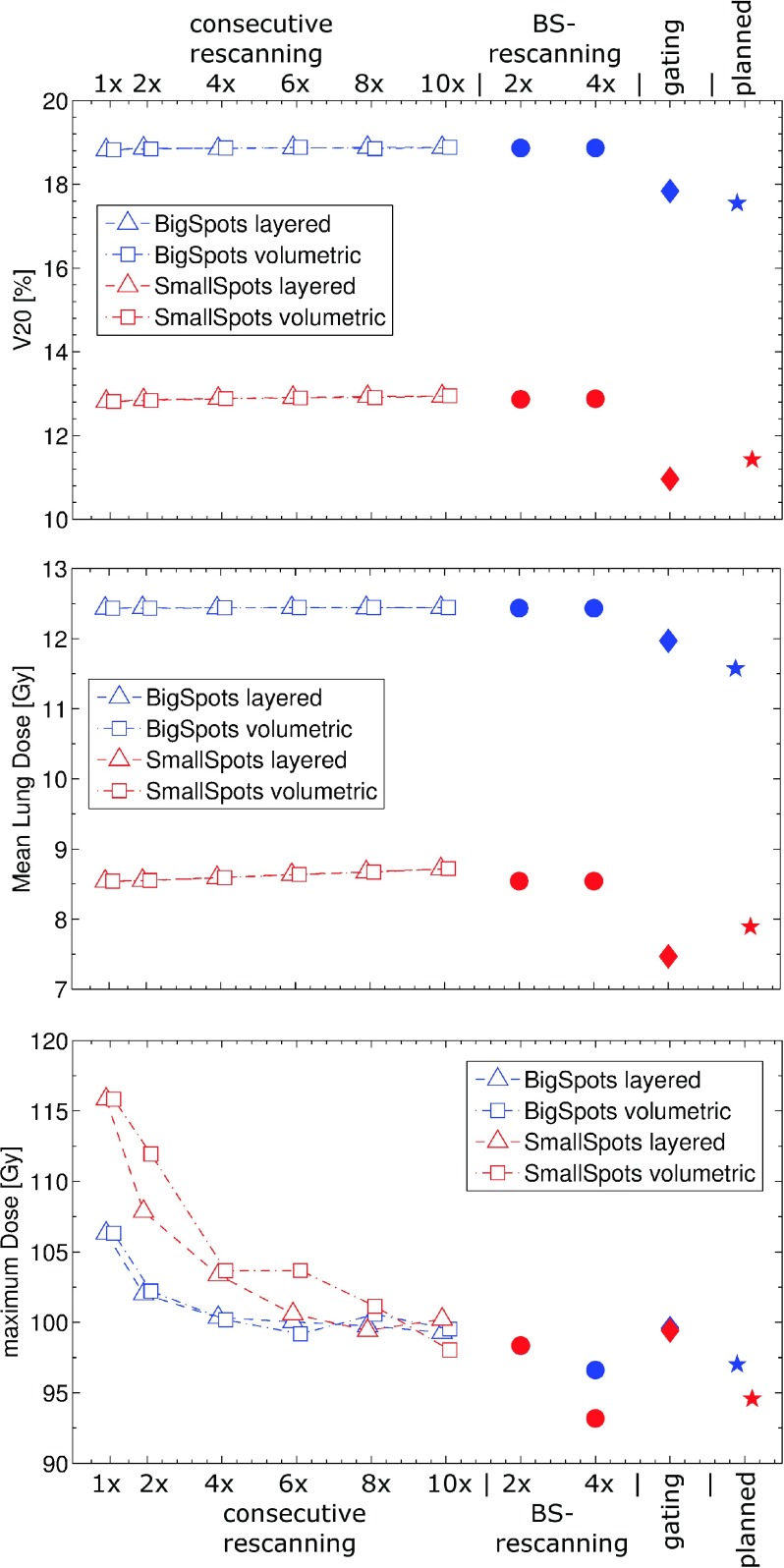
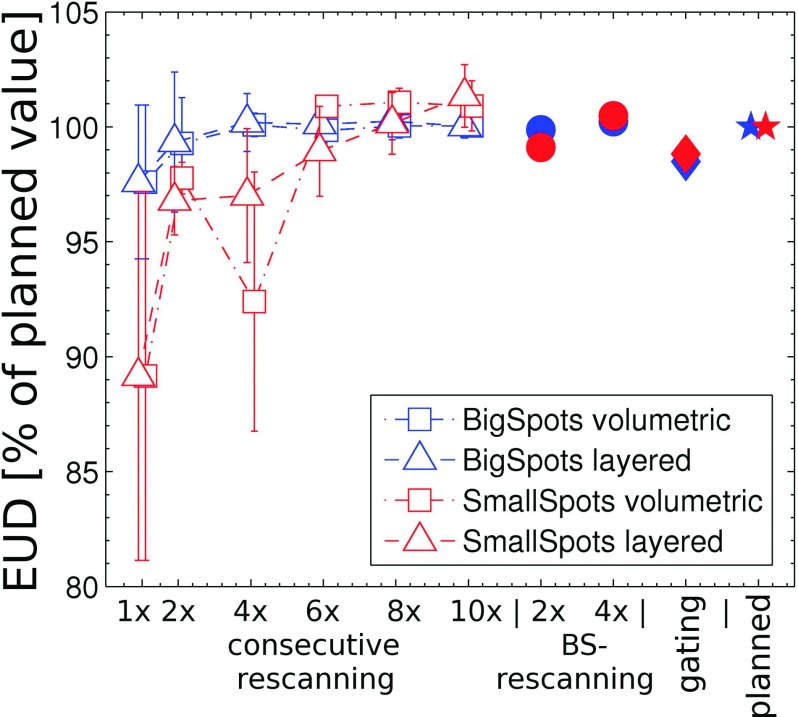
Results: For 4/5 patients, layered rescanning 6/2 times (for the small/large spot size) maintains equivalent uniform dose within the target >98% for a single fraction. Breath sampling the timing of rescanning is ∼ 2 times more effective than the same number of continuous rescans. Volumetric rescanning is sensitive to synchronization effects, which was observed in 3/5 patients, though not for layered rescanning. For the large spot size, rescanning compared favorably with gating in terms of time requirements, i.e., 2x-rescanning is on average a factor ∼ 2.6 faster than gating for this scenario. For the small spot size however, 6x-rescanning takes on average 65% longer compared to gating. Rescanning has no effect on normal lung V20 and mean lung dose (MLD), though it reduces the maximum lung dose by on average 6.9 ± 2.4/16.7 ± 12.2 Gy(RBE) for the large and small spot sizes, respectively. Gating leads to a similar reduction in maximum dose and additionally reduces V20 and MLD. Breath-sampled rescanning is most successful in reducing the maximum dose to the normal lung.
Conclusions: Both rescanning (2-6 times, depending on the beam size) as well as gating was able to mitigate interplay effects in the target for 4/5 patients studied. Layered rescanning is superior to volumetric rescanning, as the latter suffers from synchronization effects in 3/5 patients studied. Gating minimizes the irradiated volume of normal lung more efficiently, while breath-sampled rescanning is superior in reducing maximum doses to organs at risk.
Figures
References
-
- Zhang X.et al., “Intensity-modulated proton therapy reduces the dose to normal tissue compared with intensity-modulated radiation therapy or passive scattering proton therapy and enables individualized radical radiotherapy for extensive stage IIIB non-small-cell lung cancer: A virtual clinical study,” Int. J. Radiat. Oncol., Biol., Phys. 77(2), 357–366 (2010).10.1016/j.ijrobp.2009.04.028 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
