

Fibrinolysis shutdown phenotype masks changes in rodent coagulation in tissue injury versus hemorrhagic shock
- PMID: 25979440
- PMCID: PMC4492895
- DOI: 10.1016/j.surg.2015.04.008
Fibrinolysis shutdown phenotype masks changes in rodent coagulation in tissue injury versus hemorrhagic shock
Abstract
Introduction: Systemic hyperfibrinolysis (accelerated clot degradation) and fibrinolysis shutdown (impaired clot degradation) are associated with increased mortality compared with physiologic fibrinolysis after trauma. Animal models have not reproduced these changes. We hypothesize rodents have a shutdown phenotype that require an exogenous profibrinolytic to differentiate mechanisms that promote or inhibit fibrinolysis.
Methods: Fibrinolysis resistance was assessed by thrombelastography (TEG) using exogenous tissue plasminogen activator (tPA) titrations in whole blood. There were 3 experimental groups: (1) tissue injury (laparotomy/bowel crush), (2) shock (hemorrhage to mean arterial pressure of 20 mmHg), and (3) control (arterial cannulation and tracheostomy). Baseline and 30-minute postintervention blood samples were collected, and assayed with TEG challenged with taurocholic acid (TUCA).
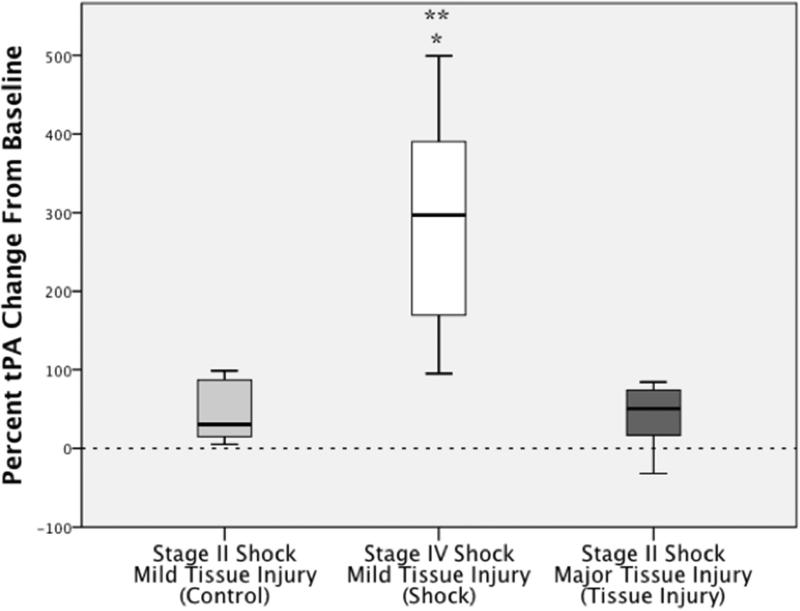
Results: Rats were resistant to exogenous tPA; the percent clot remaining 30 minutes after maximum amplitude (CL30) at 150 ng/mL (P = .511) and 300 ng/mL (P = .931) was similar to baseline, whereas 600 ng/mL (P = .046) provoked fibrinolysis. Using the TUCA challenge, the percent change in CL30 from baseline was increased in tissue injury compared with control (P = .048.), whereas CL30 decreased in shock versus control (P = .048). tPA increased in the shock group compared with tissue injury (P = .009) and control (P = .012).
Conclusion: Rats have an innate fibrinolysis shutdown phenotype. The TEG TUCA challenge is capable of differentiating changes in clot stability with rats undergoing different procedures. Tissue injury inhibits fibrinolysis, whereas shock promotes tPA-mediated fibrinolysis.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures




Similar articles
-
Shock-induced systemic hyperfibrinolysis is attenuated by plasma-first resuscitation.J Trauma Acute Care Surg. 2015 Dec;79(6):897-903; discussion 903-4. doi: 10.1097/TA.0000000000000792. J Trauma Acute Care Surg. 2015. PMID: 26680132 Free PMC article.
-
Plasma is the physiologic buffer of tissue plasminogen activator-mediated fibrinolysis: rationale for plasma-first resuscitation after life-threatening hemorrhage.J Am Coll Surg. 2015 May;220(5):872-9. doi: 10.1016/j.jamcollsurg.2015.01.026. Epub 2015 Mar 31. J Am Coll Surg. 2015. PMID: 25840538 Free PMC article.
-
Shock releases bile acid inducing platelet inhibition and fibrinolysis.J Surg Res. 2015 May 15;195(2):390-5. doi: 10.1016/j.jss.2015.01.046. Epub 2015 Jan 29. J Surg Res. 2015. PMID: 25777826 Free PMC article.
-
Temporal Changes in Fibrinolysis following Injury.Semin Thromb Hemost. 2020 Mar;46(2):189-198. doi: 10.1055/s-0039-1701016. Epub 2020 Mar 11. Semin Thromb Hemost. 2020. PMID: 32160644 Review.
-
Serine-proteases as plasminogen activators in terms of fibrinolysis.J Pharm Pharmacol. 2012 Aug;64(8):1025-39. doi: 10.1111/j.2042-7158.2012.01457.x. Epub 2012 Feb 7. J Pharm Pharmacol. 2012. PMID: 22775207 Review.
Cited by
-
A rat model of orthopedic injury-induced hypercoagulability and fibrinolytic shutdown.J Trauma Acute Care Surg. 2020 Nov;89(5):926-931. doi: 10.1097/TA.0000000000002924. J Trauma Acute Care Surg. 2020. PMID: 32890345 Free PMC article.
-
The procoagulant molecule plasminogen activator inhibitor-1 is associated with injury severity and shock in patients with and without traumatic brain injury.J Trauma Acute Care Surg. 2018 Nov;85(5):888-893. doi: 10.1097/TA.0000000000002040. J Trauma Acute Care Surg. 2018. PMID: 30086072 Free PMC article.
-
Plasma First Resuscitation Reduces Lactate Acidosis, Enhances Redox Homeostasis, Amino Acid and Purine Catabolism in a Rat Model of Profound Hemorrhagic Shock.Shock. 2016 Aug;46(2):173-82. doi: 10.1097/SHK.0000000000000588. Shock. 2016. PMID: 26863033 Free PMC article.
-
Hemorrhagic shock and tissue injury provoke distinct components of trauma-induced coagulopathy in a swine model.Eur J Trauma Emerg Surg. 2023 Apr;49(2):1079-1089. doi: 10.1007/s00068-022-02148-x. Epub 2022 Nov 1. Eur J Trauma Emerg Surg. 2023. PMID: 36319860 Free PMC article.
-
Early abnormal fibrinolysis and mortality in patients with thermal injury: a prospective cohort study.BJS Open. 2021 Mar 5;5(2):zrab017. doi: 10.1093/bjsopen/zrab017. BJS Open. 2021. PMID: 33893737 Free PMC article.
References
-
- Brohi K, Cohen MJ, Ganter MT, Schultz MJ, Levi M, Mackersie RC, et al. Acute coagulopathy of trauma: hypoperfusion induces systemic anticoagulation and hyperfibrinolysis. The Journal of trauma. 2008;64(5):1211–7. discussion 7. - PubMed
-
- Sillesen M, Rasmussen LS, Jin G, Jepsen CH, Imam A, Hwabejire JO, et al. Assessment of coagulopathy, endothelial injury, and inflammation after traumatic brain injury and hemorrhage in a porcine model. The journal of trauma and acute care surgery. 2014;76(1):12–9. discussion 9-20. - PubMed
-
- Cho SD, Holcomb JB, Tieu BH, Englehart MS, Morris MS, Karahan ZA, et al. Reproducibility of an animal model simulating complex combat-related injury in a multiple-institution format. Shock. 2009;31(1):87–96. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
