

Encephalitis and AMPA receptor antibodies: Novel findings in a case series of 22 patients
- PMID: 25979696
- PMCID: PMC4478035
- DOI: 10.1212/WNL.0000000000001682
Encephalitis and AMPA receptor antibodies: Novel findings in a case series of 22 patients
Abstract
Objective: We report the clinical features, comorbidities, and outcome of 22 newly identified patients with antibodies to the α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor (AMPAR).
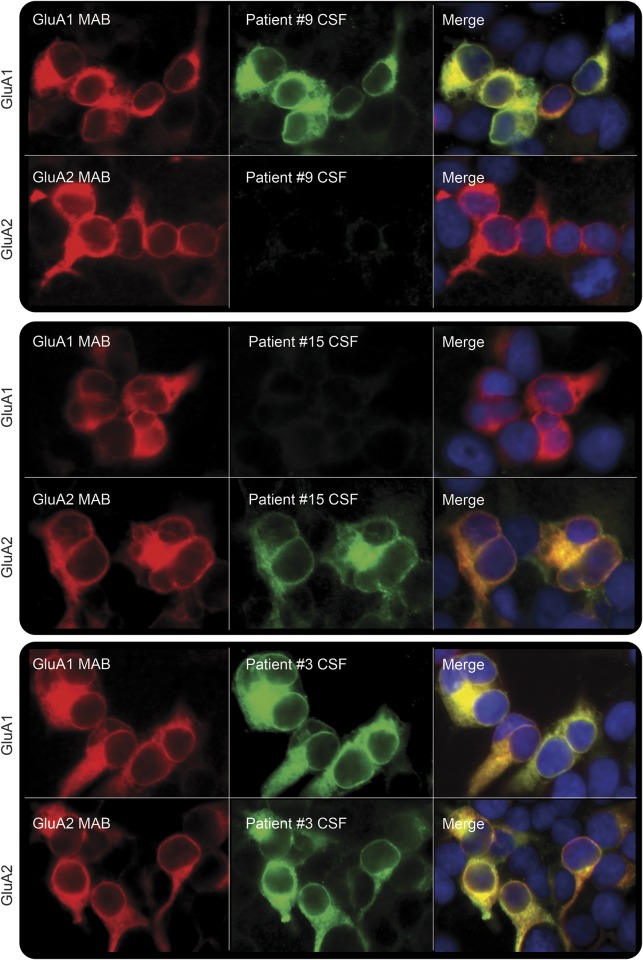
Methods: This was a retrospective review of patients diagnosed between May 2009 and March 2014. Immunologic techniques have been reported previously.
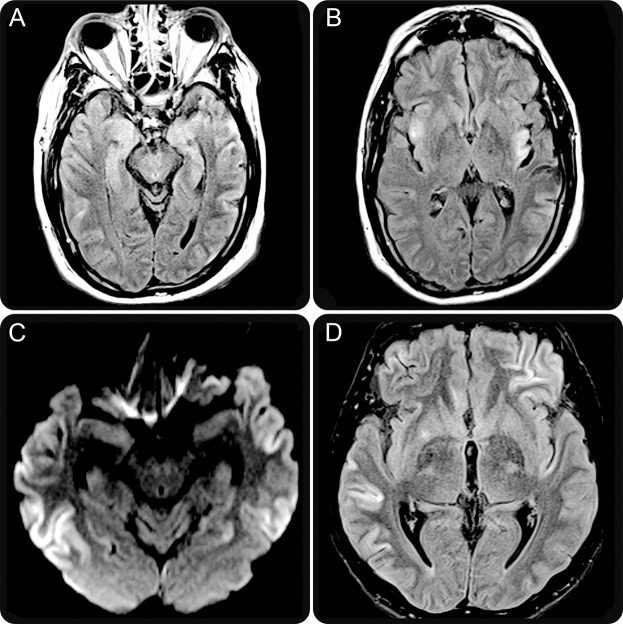
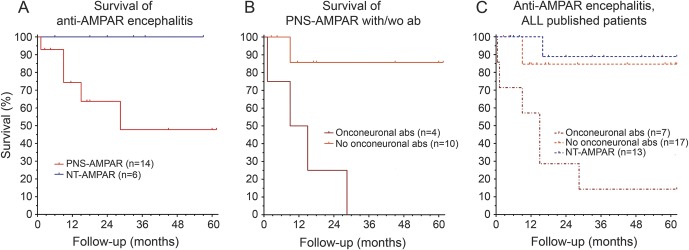
Results: Patients' median age was 62 years (range 23-81; 14 female). Four syndromes were identified: 12 (55%) patients presented with distinctive limbic encephalitis (LE), 8 (36%) with limbic dysfunction along with multifocal/diffuse encephalopathy, one with LE preceded by motor deficits, and one with psychosis with bipolar features. Fourteen patients (64%) had a tumor demonstrated pathologically (5 lung, 4 thymoma, 2 breast, 2 ovarian teratoma) or radiologically (1 lung). Additional antibodies occurred in 7 patients (3 onconeuronal, 1 tumor-related, 2 cell surface, and 1 tumor-related and cell surface), all with neurologic symptoms or tumor reflecting the concurrent autoimmunity. Treatment and outcome were available from 21 patients (median follow-up 72 weeks, range 5-266): 5 had good response to immunotherapy and tumor therapy, 10 partial response, and 6 did not improve. Eventually 5 patients died; all had a tumor or additional paraneoplastic symptoms related to onconeuronal antibodies. Coexistence of onconeuronal antibodies predicted a poor outcome (p = 0.009).
Conclusion: Anti-AMPAR encephalitis usually manifests as LE, can present with other symptoms or psychosis, and is paraneoplastic in 64% of cases. Complete and impressive neurologic improvement can occur, but most patients have partial recovery. Screening for a tumor and onconeuronal antibodies is important because their detection influences outcome.
© 2015 American Academy of Neurology.
Figures
Comment in
-
Anti-AMPA receptor encephalitis: The family of glutamatergic autoencephalitides further expands.Neurology. 2015 Jun 16;84(24):2390-1. doi: 10.1212/WNL.0000000000001693. Epub 2015 May 15. Neurology. 2015. PMID: 25979697 No abstract available.
References
-
- Sprengel R. Role of AMPA receptors in synaptic plasticity. Cell Tissue Res 2006;326:447–455. - PubMed