

Right Heart Score for Predicting Outcome in Idiopathic, Familial, or Drug- and Toxin-Associated Pulmonary Arterial Hypertension
- PMID: 25981508
- PMCID: PMC4466029
- DOI: 10.1016/j.jcmg.2014.12.029
Right Heart Score for Predicting Outcome in Idiopathic, Familial, or Drug- and Toxin-Associated Pulmonary Arterial Hypertension
Abstract
Objectives: This study sought to determine whether a simple score combining indexes of right ventricular (RV) function and right atrial (RA) size would offer good discrimination of outcome in patients with pulmonary arterial hypertension (PAH).
Background: Identifying a simple score of outcome could simplify risk stratification of patients with PAH and potentially lead to improved tailored monitoring or therapy.
Methods: We recruited patients from both Stanford University (derivation cohort) and VU University Medical Center (validation cohort). The composite endpoint for the study was death or lung transplantation. A Cox proportional hazard with bootstrap CI adjustment model was used to determine independent correlates of death or transplantation. A predictive score was developed using the beta coefficients of the multivariable models.
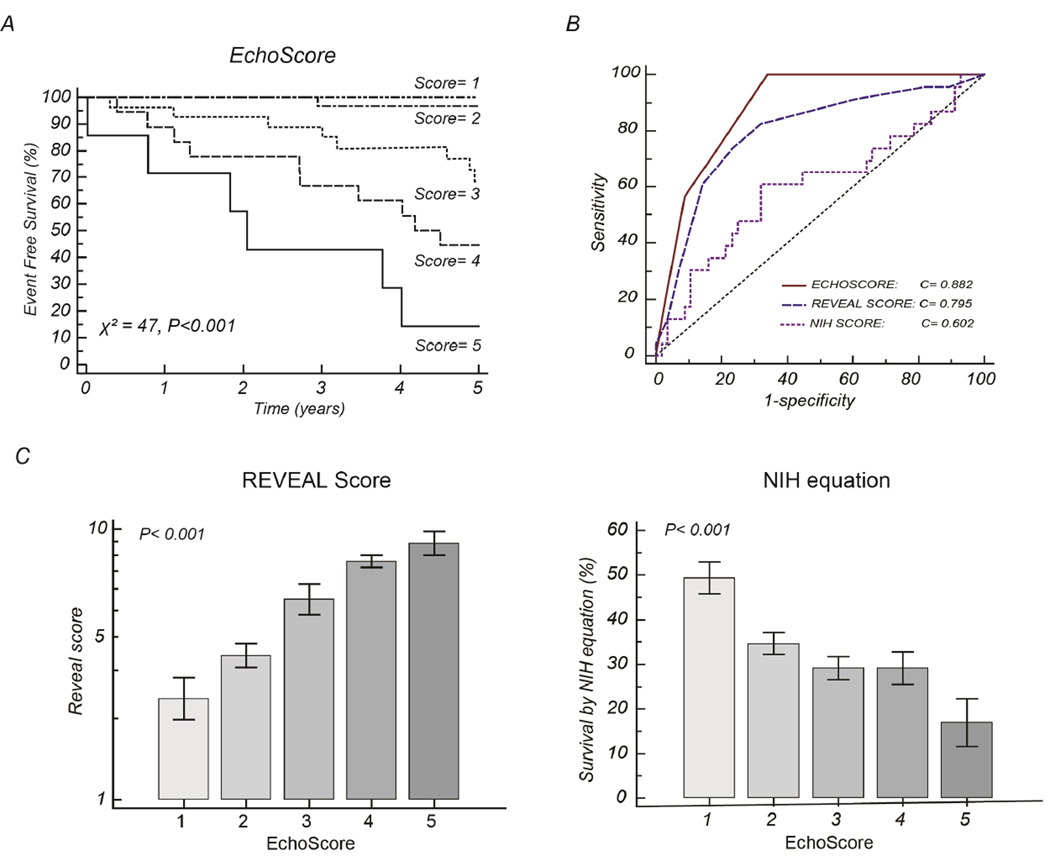
Results: For the derivation cohort (n = 95), the majority of patients were female (79%), average age was 43 ± 11 years, mean pulmonary arterial pressure was 54 ± 14 mm Hg, and pulmonary vascular resistance index was 25 ± 12 Wood units × m(2). Over an average follow-up of 5 years, the composite endpoint occurred in 34 patients, including 26 deaths and 8 patients requiring lung transplant. On multivariable analysis, RV systolic dysfunction grade (hazard ratio [HR]: 3.4 per grade; 95% confidence interval [CI]: 2.0 to 7.8; p < 0.001), severe RA enlargement (HR: 3.0; 95% CI: 1.3 to 8.1; p = 0.009), and systemic blood pressure <110 mm Hg (HR: 3.3; 95% CI: 1.5 to 9.4; p < 0.001) were independently associated with outcome. A right heart (RH) score constructed on the basis of these 3 parameters compared favorably with the National Institutes of Health survival equation (0.88; 95% CI: 0.79 to 0.94 vs. 0.60; 95% CI: 0.49 to 0.71; p < 0.001) but was not statistically different than the REVEAL (Registry to Evaluate Early and Long-Term PAH Disease Management) score c-statistic of 0.80 (95% CI: 0.69 to 0.88) with p = 0.097. In the validation cohort (n = 87), the RH score remained the strongest independent correlate of outcome.
Conclusions: In patients with prevalent PAH, a simple RH score may offer good discrimination of long-term outcome.
Keywords: atrial function; heart failure; outcome; pulmonary hypertension; right heart.
Copyright © 2015 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Predicting Mortality in Pulmonary Arterial Hypertension: Can It Really Be That Simple?JACC Cardiovasc Imaging. 2015 Jun;8(6):639-41. doi: 10.1016/j.jcmg.2015.01.021. JACC Cardiovasc Imaging. 2015. PMID: 26068282 No abstract available.
-
The Authors Reply.JACC Cardiovasc Imaging. 2016 May;9(5):630. doi: 10.1016/j.jcmg.2015.09.016. Epub 2016 Feb 17. JACC Cardiovasc Imaging. 2016. PMID: 26897682 No abstract available.
-
Right Heart Score for Predicting Outcome in PAH: Is It All Inclusive?JACC Cardiovasc Imaging. 2016 May;9(5):628-30. doi: 10.1016/j.jcmg.2015.09.015. Epub 2016 Feb 17. JACC Cardiovasc Imaging. 2016. PMID: 26897688 No abstract available.
References
-
- Humbert M, Sitbon O, Chaouat A, et al. Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hypertension in the modern management era. Circulation. 2010;122:156–163. - PubMed
-
- Benza RL, Miller DP, Gomberg-Maitland M, et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL) Circulation. 2010;122:164–172. - PubMed
-
- Vonk-Noordegraaf A, Haddad F, Chin KM, et al. Right heart adaptation to pulmonary arterial hypertension: physiology and pathobiology. Journal of the American College of Cardiology. 2013;62:D22–D33. - PubMed
-
- D'Alonzo GE, Barst RJ, Ayres SM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Annals of internal medicine. 1991;115:343–349. - PubMed
-
- van Wolferen SA, van de Veerdonk MC, Mauritz GJ, et al. Clinically significant change in stroke volume in pulmonary hypertension. Chest. 2011;139:1003–1009. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
