

Can Normal Fracture Healing Be Achieved When the Implant Is Retained on the Basis of Infection? An Experimental Animal Model
- PMID: 25981711
- PMCID: PMC4562922
- DOI: 10.1007/s11999-015-4331-9
Can Normal Fracture Healing Be Achieved When the Implant Is Retained on the Basis of Infection? An Experimental Animal Model
Abstract
Background: Infection after open fractures is a common complication. Treatment options for infections developed after intramedullary nailing surgery remain a topic of controversy. We therefore used a rat fracture model to evaluate the effects of infection on osseous union when the implant was maintained.
Questions/purposes: In a rat model, (1) does infection alter callus strength; (2) does infection alter the radiographic appearance of callus; and (3) does infection alter the histological properties of callus?
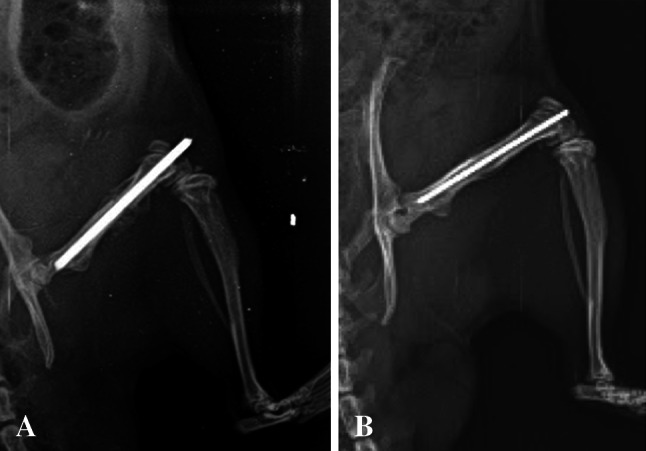
Methods: An open femoral fracture was created and fixed with an intramedullary Kirschner wire in 72 adult male Sprague-Dawley rats, which were divided into two study groups. In the infection group, the fracture site was contaminated with Staphylococcus aureus (36 animals), whereas in the control group, there was no bacterial contamination (36 animals). No antibiotics were used either for prophylaxis or for treatment. We performed biomechanical (maximum torque causing failure and stiffness), radiographic (Lane and Sandhu scoring for callus formation), and histologic (scoring for callus maturity) assessments at 3 and 6 weeks. The number of bacteria colonies on the femur, wire, and soft tissue inside knee were compared to validate that we successfully created an infection model. The number of bacteria colonies in the soft tissue inside the knee was higher in the infection group after 6 weeks than after the third week, demonstrating the presence of locally aggressive infection.
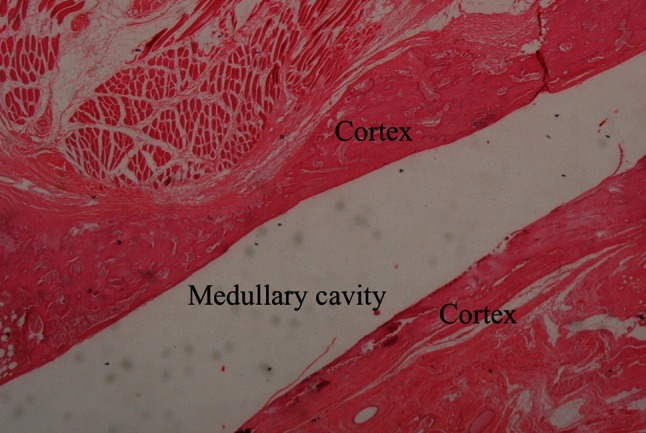
Results: Infection decreased callus strength at 6 weeks. Torque to failure (299.07 ± 65.53 Nmm versus 107.20 ± 88.81, mean difference with 95% confidence interval, 192 [43-340]; p = 0.007) and stiffness at 6 weeks (11.28 ± 2.67 Nmm versus 2.03 ± 1.68, mean difference with 95% confidence interval, 9 [3-16]; p = 0.004) both were greater in the control group than in the group with infection. Radiographic analysis at 6 weeks demonstrated the fracture line was less distinct (Lane and Sandhu score of 2-3) in the infection group and complete union was observed (Lane and Sandhu score of 3-4) in the control group (p = 0.001). Semiquantitative histology scores were not different between the noninfected controls and the rats with infection (score 10 versus 9).
Conclusions: Retaining an implant in the presence of an underlying infection without antibiotic treatment leads to weaker callus and impedes callus maturation compared with noninfected controls in a rat model. Future studies might evaluate whether antibiotic treatment would modify this result.
Clinical relevance: This model sets the stage for further investigations that might study the influence of different interventions on fracture healing in implant-associated osteomyelitis. Future observational studies might also evaluate the histological properties of callus in patients with osteomyelitis.
Figures

References
-
- Court-Brown CM, Keating JF, McQueen MM. Infection after intramedullary nailing of the tibia. Incidence and protocol for management. J Bone Joint Surg Br. 1992;74:770–774. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
