

Quantification of atrial dynamics using cardiovascular magnetic resonance: inter-study reproducibility
- PMID: 25982348
- PMCID: PMC4434799
- DOI: 10.1186/s12968-015-0140-2
Quantification of atrial dynamics using cardiovascular magnetic resonance: inter-study reproducibility
Abstract
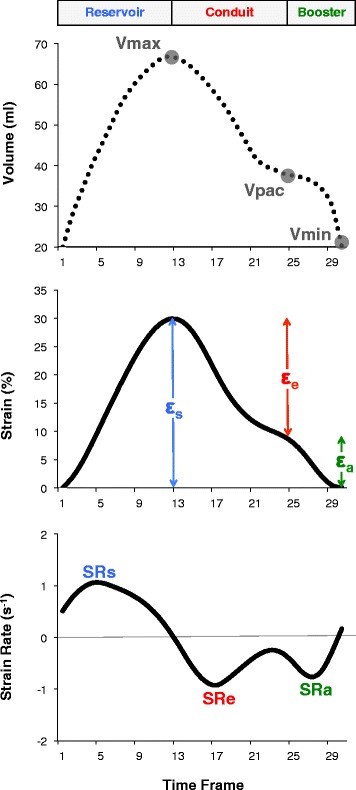
Background: Cardiovascular magnetic resonance (CMR) offers quantification of phasic atrial functions based on volumetric assessment and more recently, on CMR feature tracking (CMR-FT) quantitative strain and strain rate (SR) deformation imaging. Inter-study reproducibility is a key requirement for longitudinal studies but has not been defined for CMR-based quantification of left atrial (LA) and right atrial (RA) dynamics.
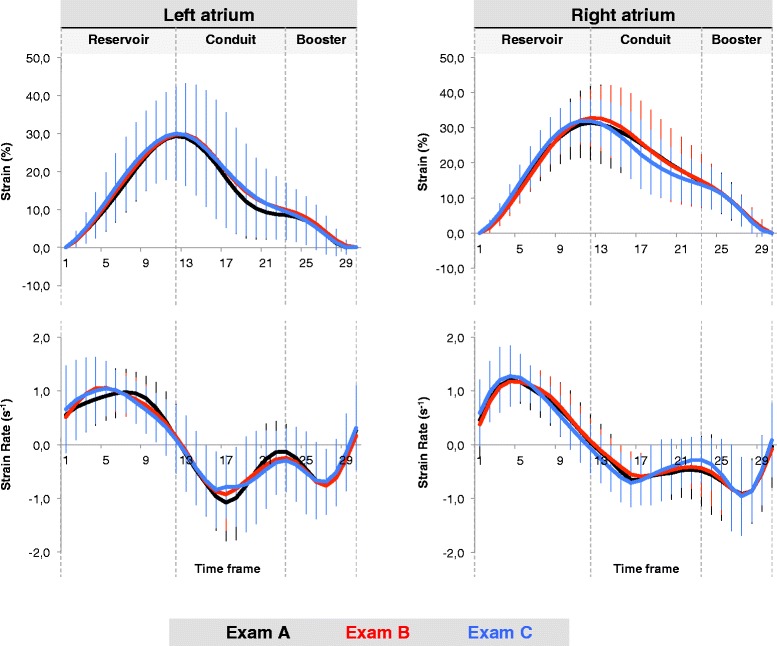
Methods: Long-axis 2- and 4-chamber cine images were acquired at 9:00 (Exam A), 9:30 (Exam B) and 14:00 (Exam C) in 16 healthy volunteers. LA and RA reservoir, conduit and contractile booster pump functions were quantified by volumetric indexes as derived from fractional volume changes and by strain and SR as derived from CMR-FT. Exam A and B were compared to assess the inter-study reproducibility. Morning and afternoon scans were compared to address possible diurnal variation of atrial function.
Results: Inter-study reproducibility was within acceptable limits for all LA and RA volumetric, strain and SR parameters. Inter-study reproducibility was better for volumetric indexes and strain than for SR parameters and better for LA than for RA dynamics. For the LA, reservoir function showed the best reproducibility (intraclass correlation coefficient (ICC) 0.94-0.97, coefficient of variation (CoV) 4.5-8.2%), followed by conduit (ICC 0.78-0.97, CoV 8.2-18.5%) and booster pump function (ICC 0.71-0.95, CoV 18.3-22.7). Similarly, for the RA, reproducibility was best for reservoir function (ICC 0.76-0.96, CoV 7.5-24.0%) followed by conduit (ICC 0.67-0.91, CoV 13.9-35.9) and booster pump function (ICC 0.73-0.90, CoV 19.4-32.3). Atrial dynamics were not measurably affected by diurnal variation between morning and afternoon scans.
Conclusions: Inter-study reproducibility for CMR-based derivation of LA and RA functions is acceptable using either volumetric, strain or SR parameters with LA function showing higher reproducibility than RA function assessment. Amongst the different functional components, reservoir function is most reproducibly assessed by either technique followed by conduit and booster pump function, which needs to be considered in future longitudinal research studies.
Figures
References
-
- Dodson JA, Neilan TG, Shah RV, Farhad H, Blankstein R, Steigner M, et al. Left atrial passive emptying function determined by cardiac magnetic resonance predicts atrial fibrillation recurrence after pulmonary vein isolation. Circ Cardiovasc Imaging. 2014;7:586–92. doi: 10.1161/CIRCIMAGING.113.001472. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
