

Dendritic cells transfected with heat-shock protein 70 messenger RNA for patients with hepatitis C virus-related hepatocellular carcinoma: a phase 1 dose escalation clinical trial
- PMID: 25982372
- PMCID: PMC11028566
- DOI: 10.1007/s00262-015-1709-1
Dendritic cells transfected with heat-shock protein 70 messenger RNA for patients with hepatitis C virus-related hepatocellular carcinoma: a phase 1 dose escalation clinical trial
Abstract
Background: We previously reported overexpression of heat-shock protein (HSP) 70 in hepatitis C virus (HCV)-related hepatocellular carcinoma (HCC) using proteomic profiling and immunohistochemical staining (IHS). This suggested that HSP70 could be a molecular target for treatment of HCC.
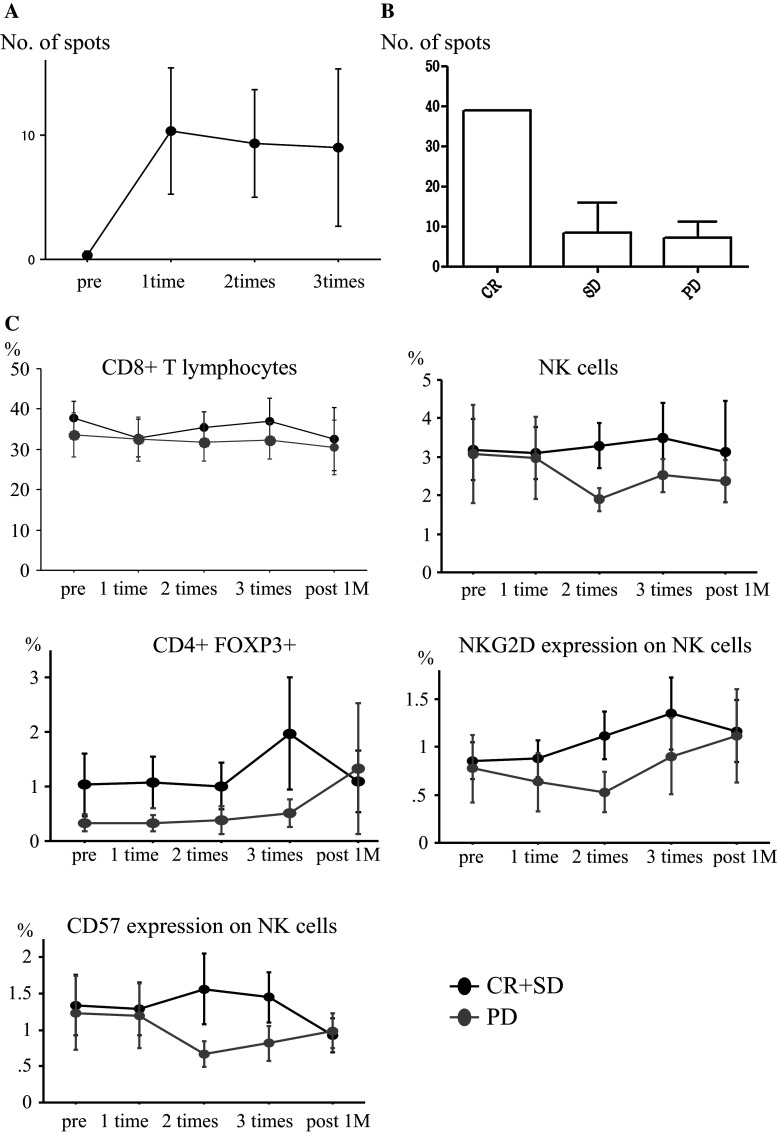
Methods: Twelve patients with HCV-related HCC were enrolled in a phase 1 clinical trial. Dendritic cells (DCs) transfected with HSP70 mRNA (HSP70-DCs) induced by electroporation were injected intradermally. Patients were treated three times every 3 weeks. The number of HSP70-DCs injected was 1 × 10(7) as the lowest dose, then 2 × 10(7) as the medium dose, and then 3 × 10(7) as the highest dose. Immunological analyses were performed.
Findings: No adverse effects of grade III/IV, except one grade III liver abscess at the 3 × 10(7) dose, were observed. Thus, we added three more patients to confirm whether 3 × 10(7) is an appropriate dose. Eventually, we chose 3 × 10(7) as the recommended dose of DCs. Complete response (CR) without any recurrence occurred in two patients, stable disease in five, and progression of disease in five. The two patients with CR have had no recurrence for 44 and 33 months, respectively. IHS in one patient who underwent partial hepatectomy showed infiltration of CD8+ T cells and granzyme B in tumors, indicating that the dominant immune effector cells were cytotoxic T lymphocytes with tumor-killing activity.
Interpretation: This study demonstrated that HSP70-DCs therapy is both safe and feasible in patients with HCV-related HCC. Further clinical trials should be considered.
Conflict of interest statement
The authors have no conflict of interest.
Figures



References
-
- Ohishi W, Kitamoto M, Aikata H, Kamada K, Kawakami Y, Ishihara H, Kamiyasu M, Nakanishi T, Tazuma S, Chayama K. Impact of aging on the development of hepatocellular carcinoma in patients with hepatitis C virus infection in Japan. Scand J Gastroenterol. 2003;38(8):894–900. doi: 10.1080/00365520310004434. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
