

Disruption in proprioception from long-term thalamic deep brain stimulation: a pilot study
- PMID: 25983689
- PMCID: PMC4416461
- DOI: 10.3389/fnhum.2015.00244
Disruption in proprioception from long-term thalamic deep brain stimulation: a pilot study
Abstract
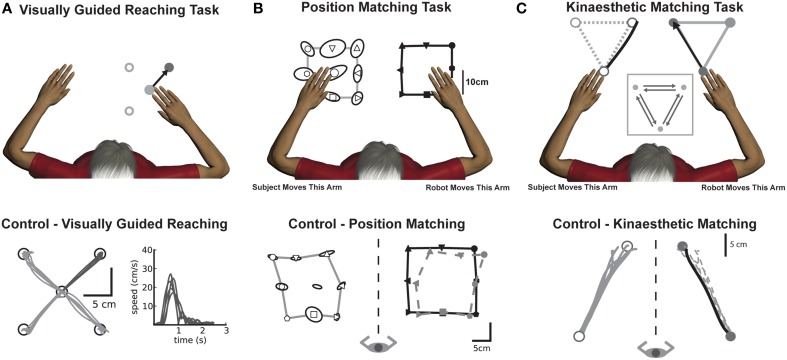
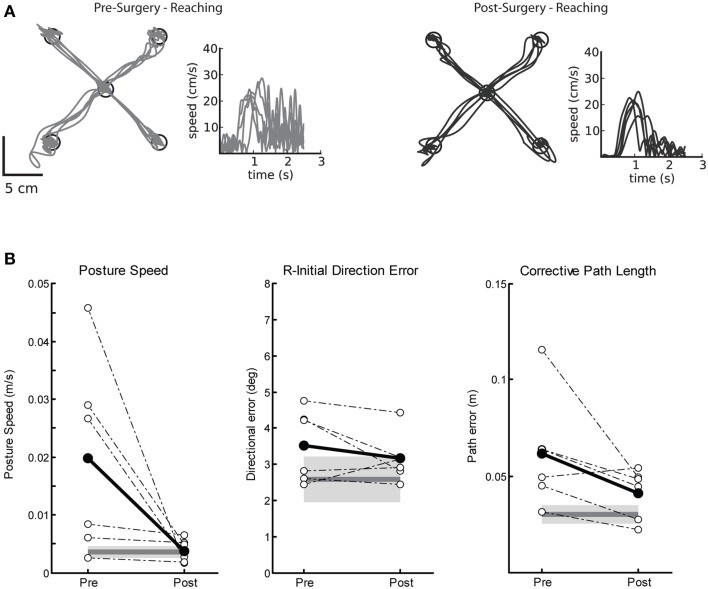
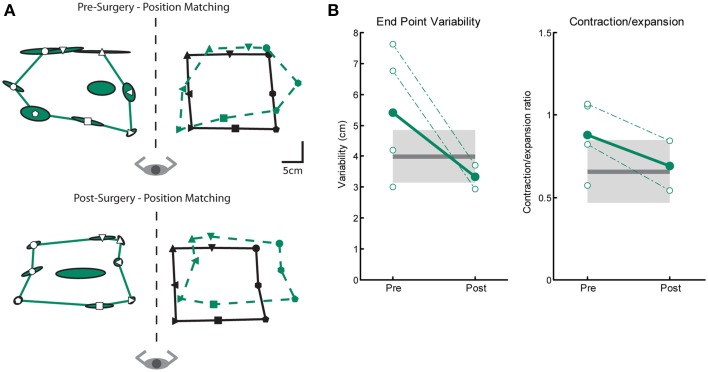
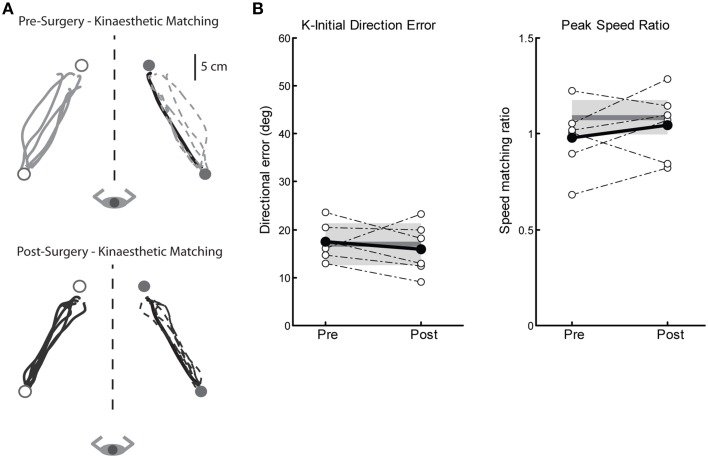
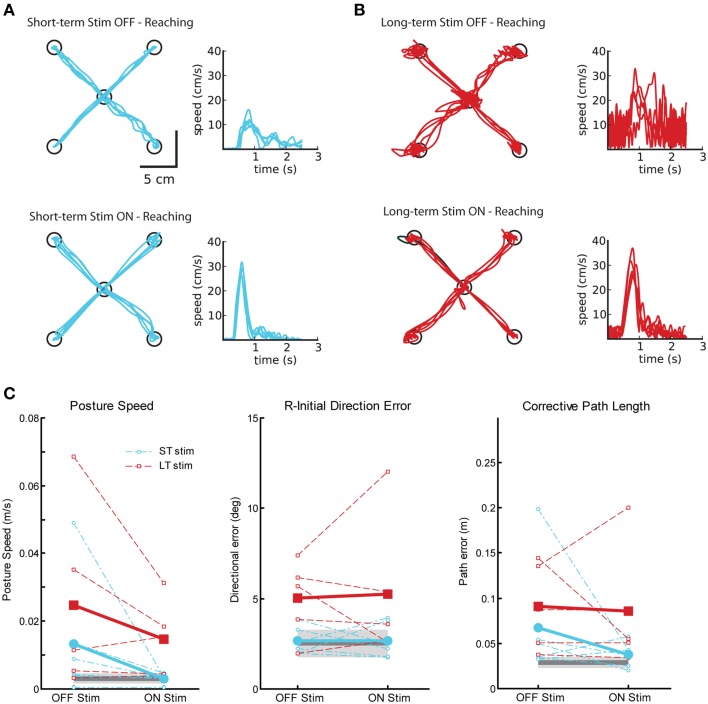
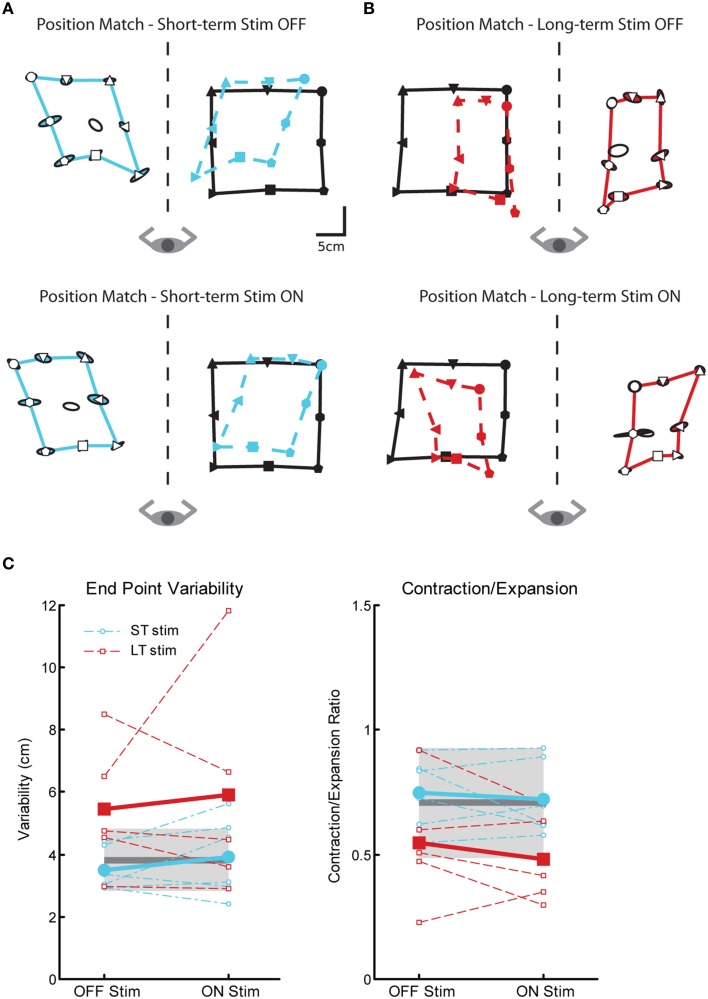
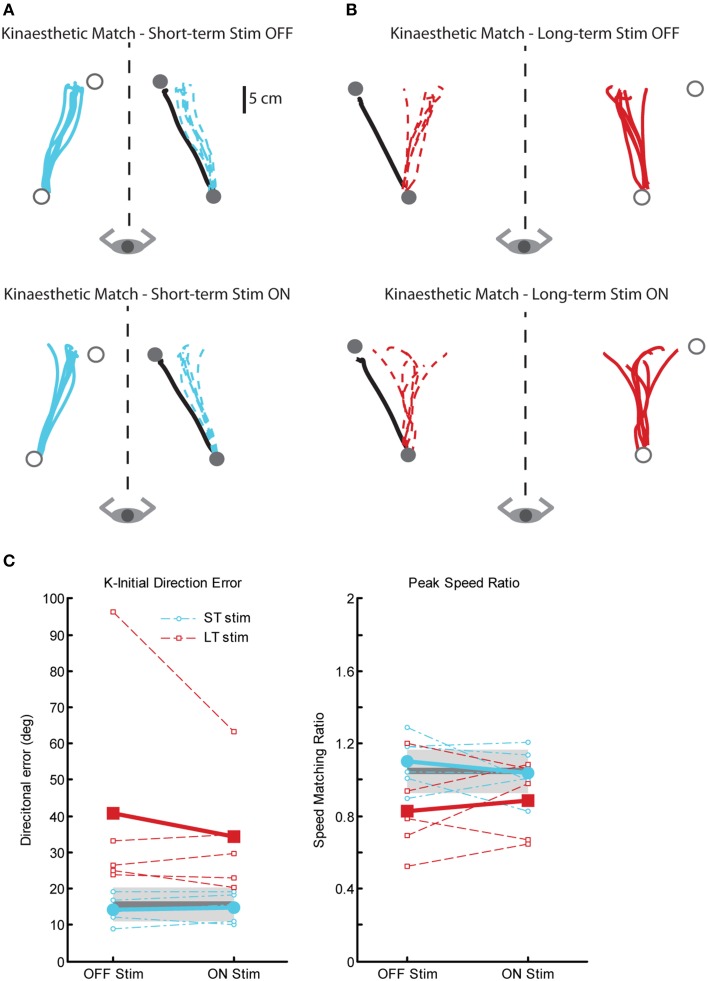
Deep brain stimulation (DBS) is an excellent treatment for tremor and is generally thought to be reversible by turning off stimulation. For tremor, DBS is implanted in the ventrointermedius (Vim) nucleus of the thalamus, a region that relays proprioceptive information for movement sensation (kinaesthesia). Gait disturbances have been observed with bilateral Vim DBS, but the long-term effects on proprioceptive processing are unknown. We aimed to determine whether Vim DBS surgical implantation or stimulation leads to proprioceptive deficits in the upper limb. We assessed two groups of tremor subjects on measures of proprioception (kinaesthesia, position sense) and motor function using a robotic exoskeleton. In the first group (Surgery), we tested patients before and after implantation of Vim DBS, but before DBS was turned on to determine if proprioceptive deficits were inherent to tremor or caused by DBS implantation. In the second group (Stim), we tested subjects with chronically implanted Vim DBS ON and OFF stimulation. Compared to controls, there were no proprioceptive deficits before or after DBS implantation in the Surgery group. Surprisingly, those that received chronic long-term stimulation (LT-stim, 3-10 years) displayed significant proprioceptive deficits ON and OFF stimulation not present in subjects with chronic short-term stimulation (ST-stim, 0.5-2 years). LT-stim had significantly larger variability and reduced workspace area during the position sense assessment. During the kinesthetic assessment, LT-stim made significantly larger directional errors and consistently underestimated the speed of the robot, despite generating normal movement speeds during motor assessment. Chronic long-term Vim DBS may potentially disrupt proprioceptive processing, possibly inducing irreversible plasticity in the Vim nucleus and/or its network connections. Our findings in the upper limb may help explain some of the gait disturbances seen by others following Vim DBS.
Keywords: deep brain stimulation (DBS); kinesthesia; position sense; proprioception; sensorimotor; tremor.
Figures
References
-
- Beuter A., Titcombe M. S., Richer F., Gross C., Guehl D. (2001). Effect of deep brain stimulation on amplitude and frequency characteristics of rest tremor in parkinson's disease. Thalamus Relat. Syst. 1, 203–211 10.1016/S1472-9288(01)00020-6 - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous