

Secondary hyperparathyroidism disease stabilization following calcimimetic therapy
- PMID: 25983950
- PMCID: PMC4421156
- DOI: 10.1093/ndtplus/sfm039
Secondary hyperparathyroidism disease stabilization following calcimimetic therapy
Abstract
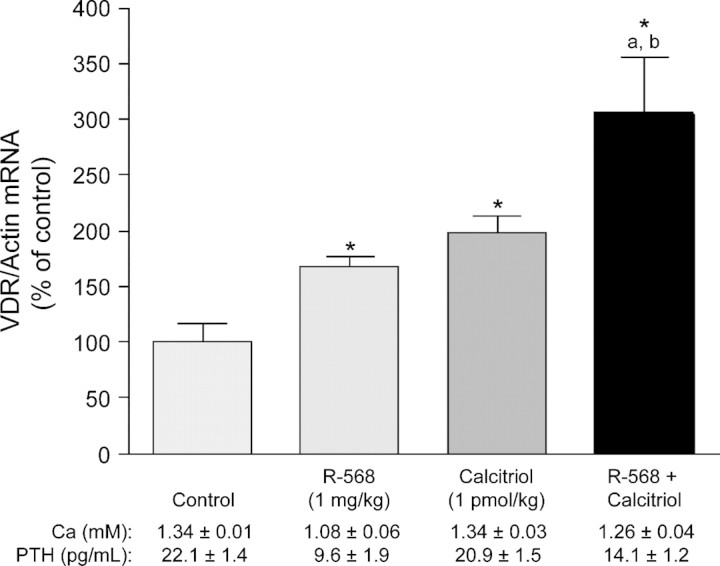
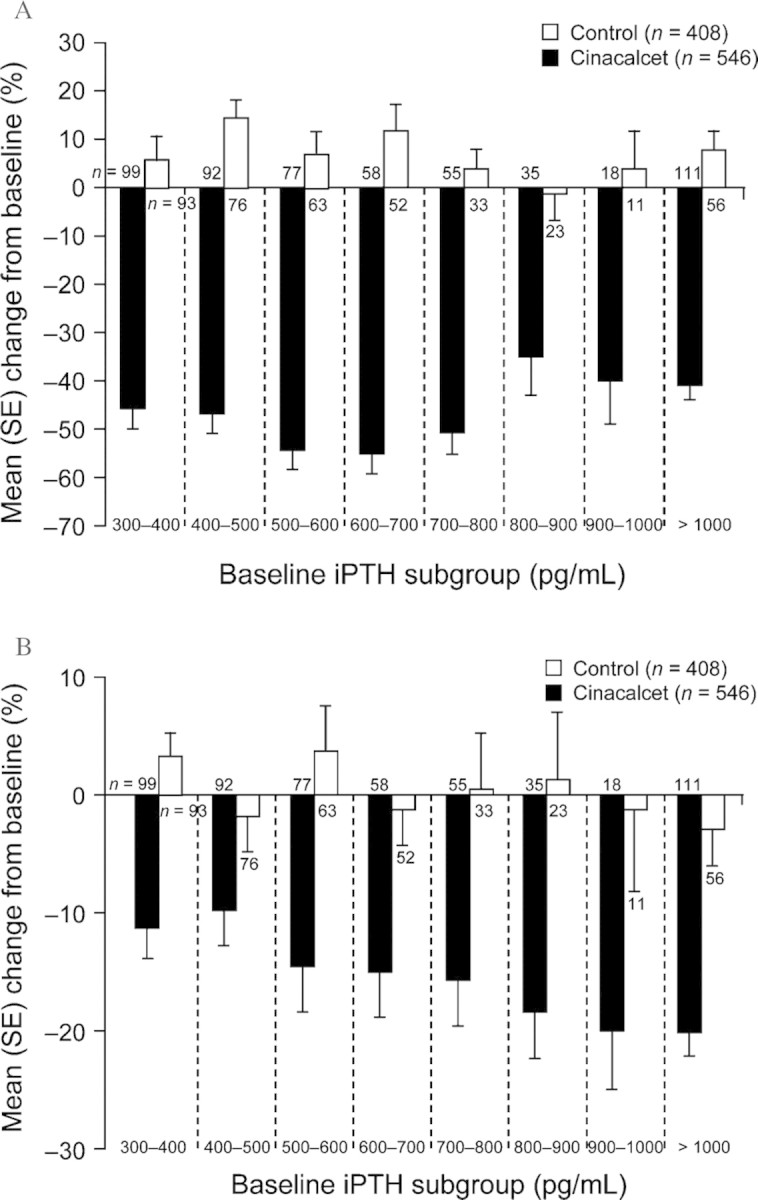
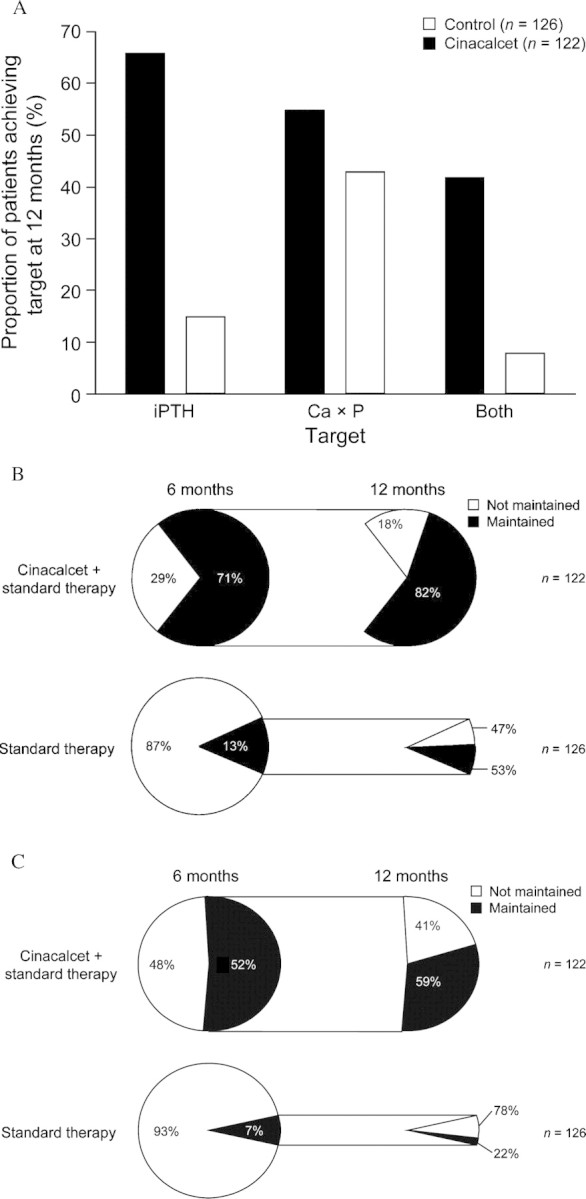
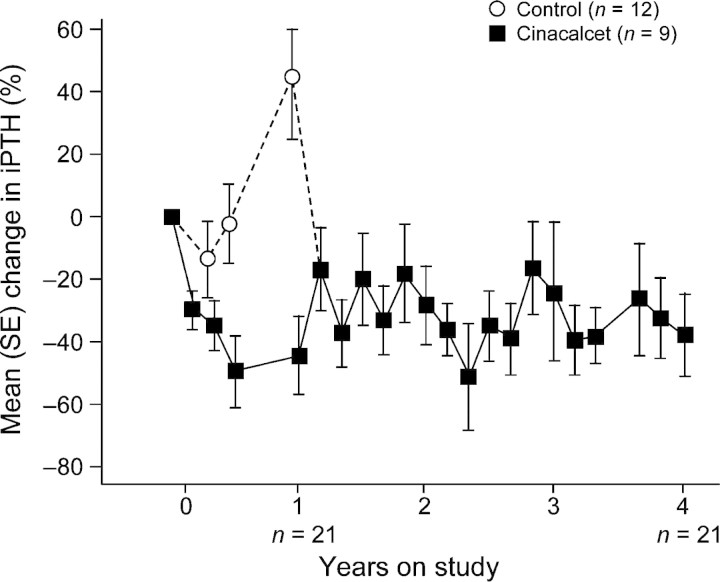
Standard therapy for secondary hyperparathyroidism (SHPT) includes dietary calcium supplementation, active vitamin D, and phosphate binders; however, these are often insufficient to allow patients to achieve their serum parathyroid hormone (PTH), calcium and calcium-phosphorus product (Ca × P) targets. Recent preclinical studies have demonstrated that treatment with type II calcimimetics that increase the sensitivity of the calcium-sensing receptor (CaR) to calcium can reverse the alterations in CaR and vitamin D receptor expression and parathyroid cell proliferation that are associated with SHPT. These data suggest that calcimimetic treatment could stabilize disease progression and improve maintenance of treatment goals. In clinical trials involving SHPT patients, the calcimimetic cinacalcet has been shown to decrease PTH, calcium, phosphorus and Ca × P. Significant improvements were seen regardless of initial disease severity, and benefits were maintained over the course of long-term therapy (up to 4 years), indicating effective disease stabilization. In conclusion, preclinical and clinical data provide both theoretical and empirical support for the use of calcimimetics in moderate and advanced SHPT to effectively stabilize disease.
Keywords: calcimimetic; calcium-sensing receptor; cinacalcet; secondary hyperparathyroidism.
Figures
References
-
- Hammerland LG, Garrett JE, Hung BC, et al. Allosteric activation of the Ca2+ receptor expressed in Xenopus laevis oocytes by NPS 467 or NPS 568. Mol Pharmacol. 1998;53:1083–1088. - PubMed
-
- Mizobuchi M, Hatamura I, Ogata H, et al. Calcimimetic compound upregulates decreased calcium-sensing receptor expression level in parathyroid glands of rats with chronic renal insufficiency. J Am Soc Nephrol. 2004;15:2579–2587. - PubMed
-
- Kifor O, Moore FD, Jr, Wang P, et al. Reduced immunostaining for the extracellular Ca2+-sensing receptor in primary and uremic secondary hyperparathyroidism. J Clin Endocrinol Metab. 1996;81:1598–1606. - PubMed
-
- Lindberg JS, Moe SM, Goodman WG, et al. The calcimimetic AMG 073 reduces parathyroid hormone and calcium × phosphorus in secondary hyperparathyroidism. Kidney Int. 2003;63:248–254. - PubMed
-
- Lindberg JS, Culleton B, Wong G, et al. Cinacalcet HCl, an oral calcimimetic agent for the treatment of secondary hyperparathyroidism in hemodialysis and peritoneal dialysis: a randomized, double-blind, multicenter study. J Am Soc Nephrol. 2005;16:800–807. - PubMed
LinkOut - more resources
Full Text Sources