

A comprehensive database of the geographic spread of past human Ebola outbreaks
- PMID: 25984346
- PMCID: PMC4432636
- DOI: 10.1038/sdata.2014.42
A comprehensive database of the geographic spread of past human Ebola outbreaks
Abstract
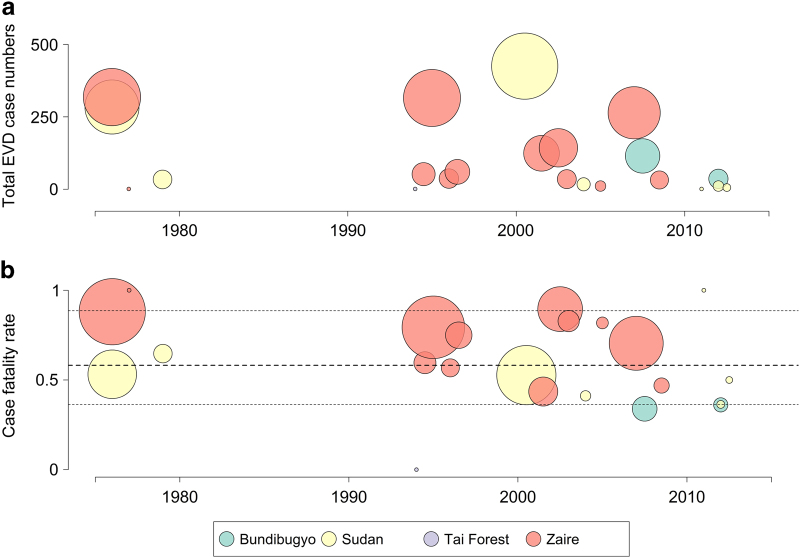
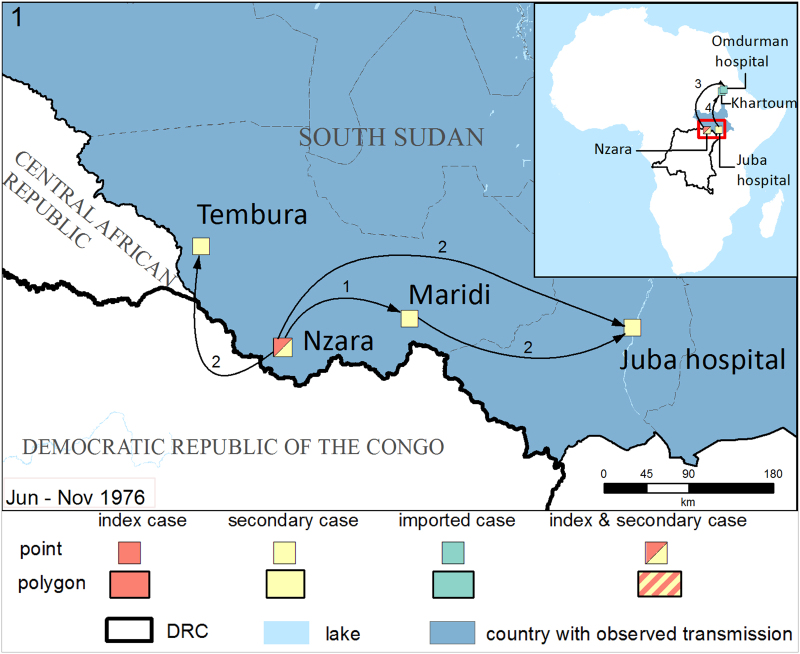
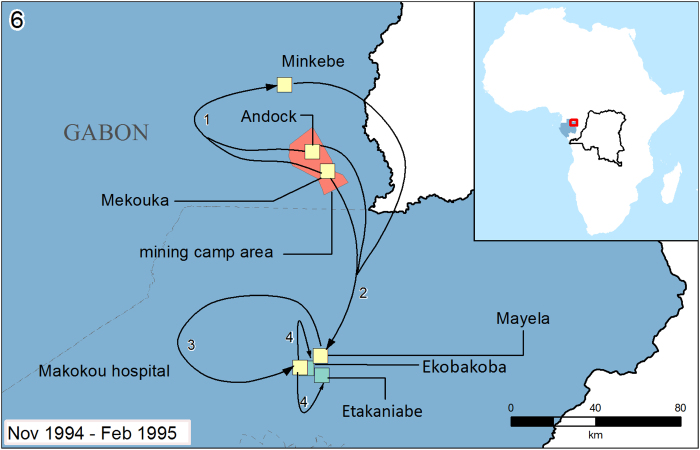
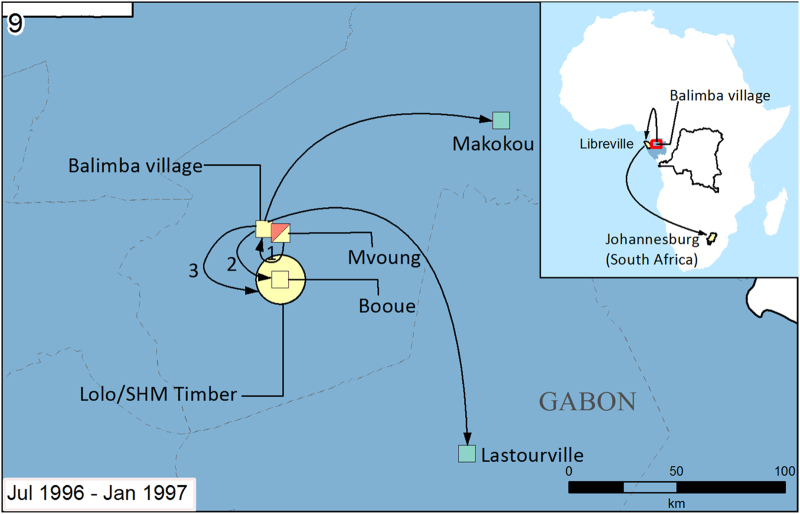
Ebola is a zoonotic filovirus that has the potential to cause outbreaks of variable magnitude in human populations. This database collates our existing knowledge of all known human outbreaks of Ebola for the first time by extracting details of their suspected zoonotic origin and subsequent human-to-human spread from a range of published and non-published sources. In total, 22 unique Ebola outbreaks were identified, composed of 117 unique geographic transmission clusters. Details of the index case and geographic spread of secondary and imported cases were recorded as well as summaries of patient numbers and case fatality rates. A brief text summary describing suspected routes and means of spread for each outbreak was also included. While we cannot yet include the ongoing Guinea and DRC outbreaks until they are over, these data and compiled maps can be used to gain an improved understanding of the initial spread of past Ebola outbreaks and help evaluate surveillance and control guidelines for limiting the spread of future epidemics.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
References
Data Citations
-
- Mylne A. 2014. Figshare. http://dx.doi.org/10.6084/m9.figshare.1168886 - DOI
References
-
- Barrette R. W. et al. Discovery of swine as a host for the Reston ebolavirus. Science 325, 204–206 (2009). - PubMed
-
- Le Guenno B. et al. Isolation and partial characterisation of a new strain of Ebola virus. The Lancet 345, 1271–1274 (1995). - PubMed
-
- King A. M., Adams M. J., Lefkowitz E. J. & Carstens E. B. Virus Taxonomy: Classification and Nomenclature of Viruses: Ninth Report of the International Committee on Taxonomy of Viruses Vol. 9. (Elsevier, 2012).
-
- Kuhn J. & Calisher C. H. Filoviruses: A Compendium of 40 Years of Epidemiological, Clinical, and Laboratory Studies 1st edn, Vol. 20 (Springer, 2008). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
