

Heterogeneity of prognostic studies of 24-hour blood pressure variability: systematic review and meta-analysis
- PMID: 25984791
- PMCID: PMC4435972
- DOI: 10.1371/journal.pone.0126375
Heterogeneity of prognostic studies of 24-hour blood pressure variability: systematic review and meta-analysis
Abstract
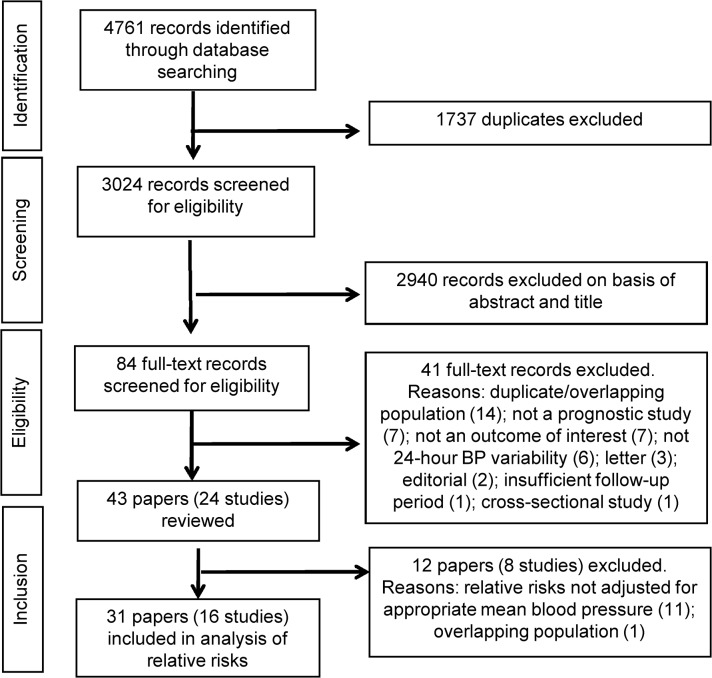
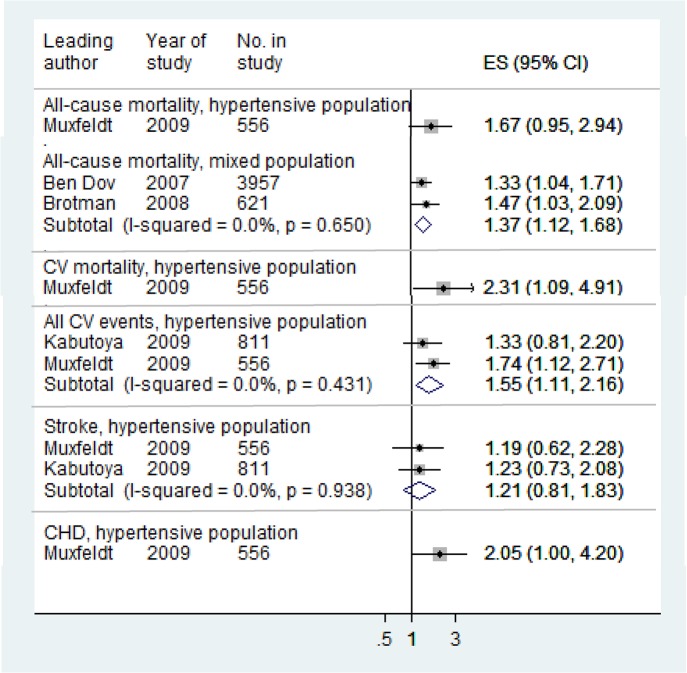
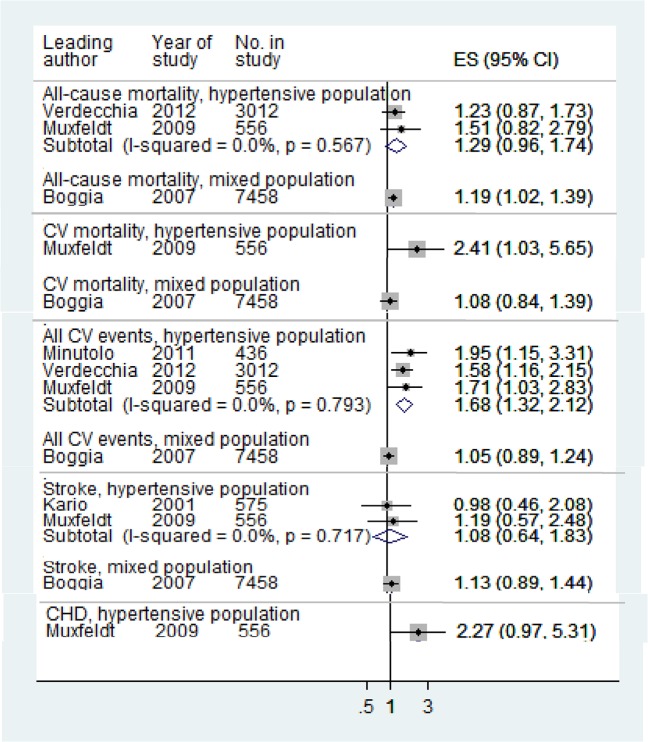
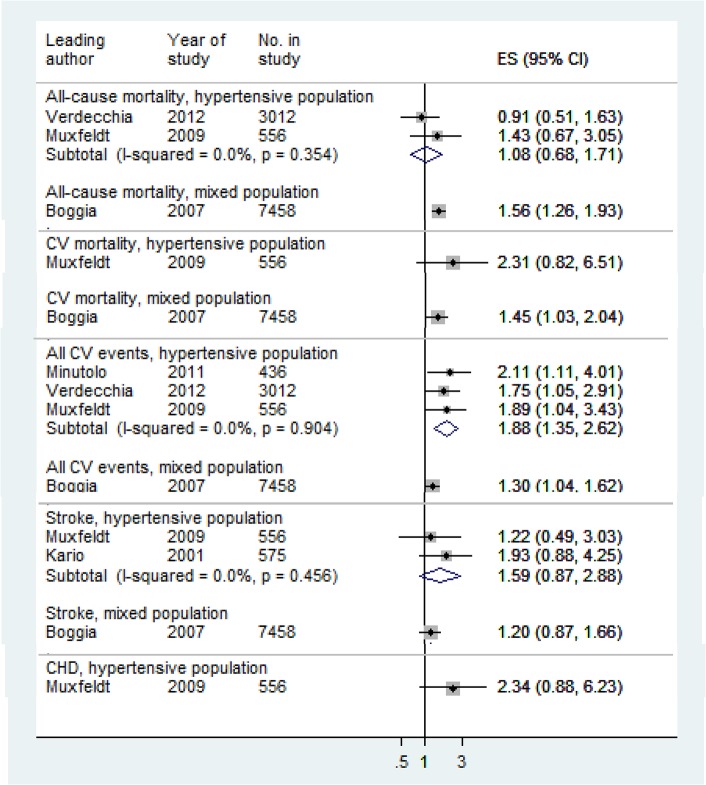
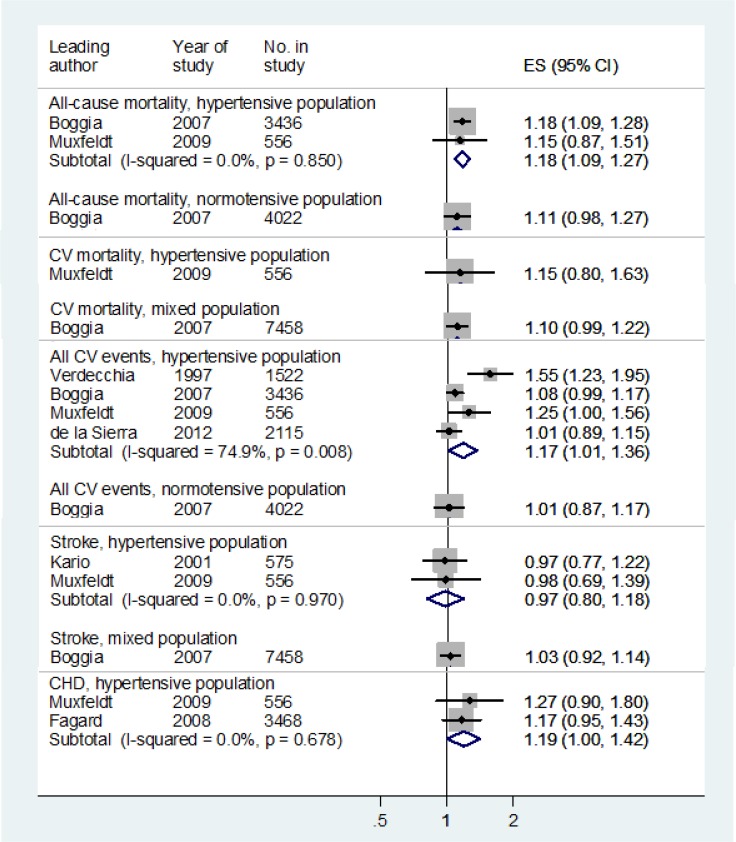
In addition to mean blood pressure, blood pressure variability is hypothesized to have important prognostic value in evaluating cardiovascular risk. We aimed to assess the prognostic value of blood pressure variability within 24 hours. Using MEDLINE, EMBASE and Cochrane Library to April 2013, we conducted a systematic review of prospective studies of adults, with at least one year follow-up and any day, night or 24-hour blood pressure variability measure as a predictor of one or more of the following outcomes: all-cause mortality, cardiovascular mortality, all cardiovascular events, stroke and coronary heart disease. We examined how blood pressure variability is defined and how its prognostic use is reported. We analysed relative risks adjusted for covariates including the appropriate mean blood pressure and considered the potential for meta-analysis. Our analysis of methods included 24 studies and analysis of predictions included 16 studies. There were 36 different measures of blood pressure variability and 13 definitions of night- and day-time periods. Median follow-up was 5.5 years (interquartile range 4.2-7.0). Comparing measures of dispersion, coefficient of variation was less well researched than standard deviation. Night dipping based on percentage change was the most researched measure and the only measure for which data could be meaningfully pooled. Night dipping or lower night-time blood pressure was associated with lower risk of cardiovascular events. The interpretation and use in clinical practice of 24-hour blood pressure variability, as an important prognostic indicator of cardiovascular events, is hampered by insufficient evidence and divergent methodologies. We recommend greater standardisation of methods.
Conflict of interest statement
Figures
References
-
- Kannel WB, Sorlie P, Gordon T. Labile hypertension: a faulty concept? The Framingham study. Circulation. 1980; 61: 1183–87. - PubMed
-
- Grove JS, Reed DM, Yano K, Hwang L. Variability in systolic blood pressure—a risk factor for coronary heart disease? Am J Epidemiol. 1997; 145: 771–6. - PubMed
-
- Sega R, Cesana G, Bombelli M, Grassi G, Stella ML, Zanchetti A, et al. Seasonal variations in home and ambulatory blood pressure in the PAMELA population. J Hypertens. 1998; 16: 1585–92. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
