

Could CCI or FBCI Fully Eliminate the Impact of Curve Flexibility When Evaluating the Surgery Outcome for Thoracic Curve Idiopathic Scoliosis Patient? A Retrospective Study
- PMID: 25984945
- PMCID: PMC4436022
- DOI: 10.1371/journal.pone.0126380
Could CCI or FBCI Fully Eliminate the Impact of Curve Flexibility When Evaluating the Surgery Outcome for Thoracic Curve Idiopathic Scoliosis Patient? A Retrospective Study
Abstract
Purpose: To clarify if CCI or FBCI could fully eliminate the influence of curve flexibility on the coronal correction rate.
Methods: We reviewed medical record of all thoracic curve AIS cases undergoing posterior spinal fusion with all pedicle screw systems from June 2011 to July 2013. Radiographical data was collected and calculated. Student t test, Pearson correlation analysis and linear regression analysis were used to analyze the data.
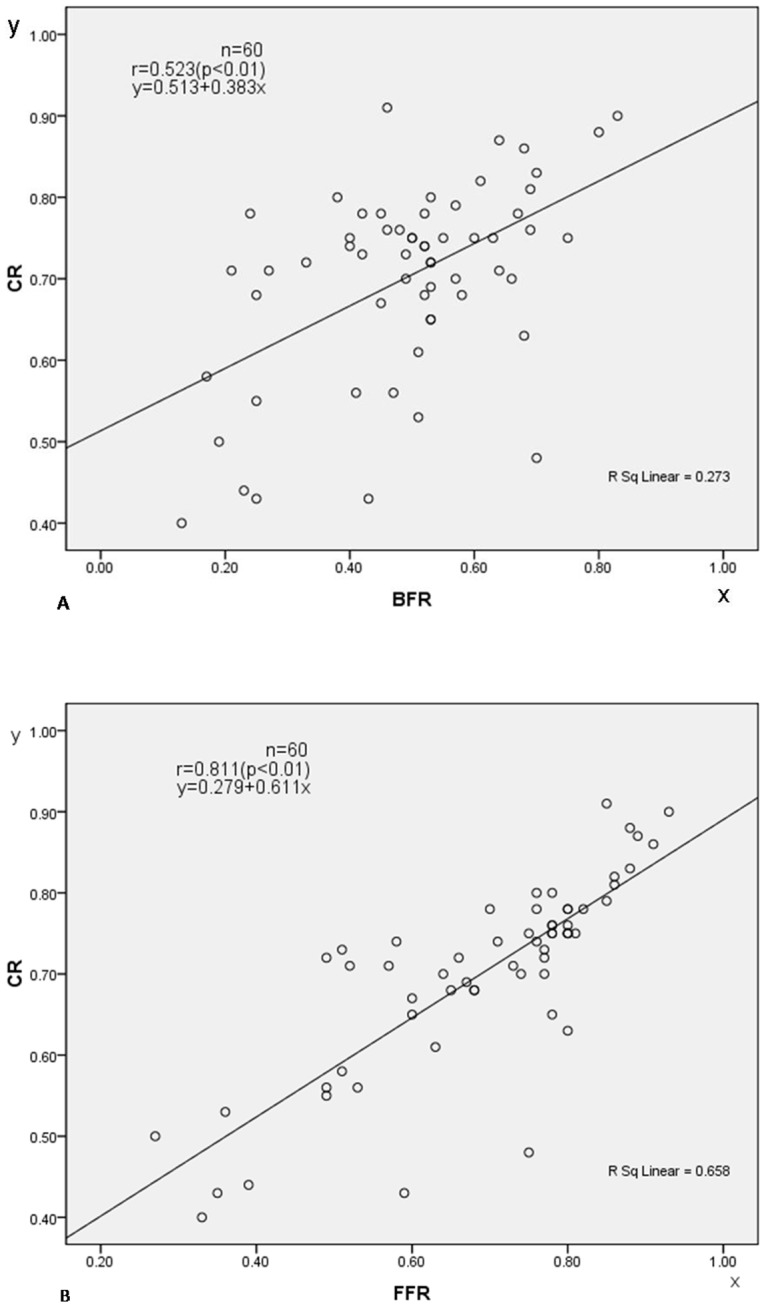
Results: 60 were included in this study. The mean age was 14.7 y (10-18 y) with 10 males (17%) and 50 females (83%). The average Risser sign was 2.7. The mean thoracic Cobb angle before operation was 51.9°. The mean bending Cobb angle was 27.6° and the mean fulcrum bending Cobb angle was 17.4°. The mean Cobb angle at 2 week after surgery was 16.3°. The Pearson correlation coefficient r between CCI and BFR was -0.856(P<0.001), and between FBCI and FFR was -0.728 (P<0.001). A modified FBCI (M-FBCI) = (CR-0.513)/BFR or a modified CCI (M-CCI) = (CR-0.279)/FFR was generated by curve estimation has no significant correlation with FFR (r=-0.08, p=0.950) or with BFR (r=0.123, p=0.349).
Conclusions: Fulcrum-bending radiographs may better predict the outcome of AIS coronal correction than bending radiographs in thoracic curveAIS patients. Neither CCI nor FBCI can fully eliminate the impact of curve flexibility on the outcome of correction. A modified CCI or FBCI can better evaluating the corrective effects of different surgical techniques or instruments.
Conflict of interest statement
Figures

Similar articles
-
Prediction of scoliosis correction with thoracic segmental pedicle screw constructs using fulcrum bending radiographs.Spine (Phila Pa 1976). 2010 Mar 1;35(5):557-61. doi: 10.1097/BRS.0b013e3181b9cfa9. Spine (Phila Pa 1976). 2010. PMID: 20118839
-
[Changhai fulcrum bending radiographic technique to assess curve flexibility in patients with adolescent idiopathic scoliosis].Zhonghua Wai Ke Za Zhi. 2014 May;52(5):355-60. Zhonghua Wai Ke Za Zhi. 2014. PMID: 25034743 Chinese.
-
The "X-Factor" index: a new parameter for the assessment of adolescent idiopathic scoliosis correction.Eur Spine J. 2011 Jan;20(1):144-50. doi: 10.1007/s00586-010-1534-3. Epub 2010 Aug 17. Eur Spine J. 2011. PMID: 20714756 Free PMC article.
-
Predictability of the fulcrum bending radiograph in scoliosis correction with alternate-level pedicle screw fixation.J Bone Joint Surg Am. 2010 Jan;92(1):169-76. doi: 10.2106/JBJS.H.01831. J Bone Joint Surg Am. 2010. PMID: 20048109 Clinical Trial.
-
Prediction of Curve Correction Using Alternate Level Pedicle Screw Placement in Patients With Adolescent Idiopathic Scoliosis (AIS) Lenke 1 and 2 Using Supine Side Bending (SB) and Fulcrum Bending (FB) Radiograph.Spine (Phila Pa 1976). 2015 Oct 15;40(20):1605-12. doi: 10.1097/BRS.0000000000001087. Spine (Phila Pa 1976). 2015. PMID: 26261915
Cited by
-
Supine Traction vs Fulcrum Bending Radiographs in Preoperative Imaging of Scoliosis Patients Treated With Magnetically Controlled Growing Rods (MCGR) - which Technique is Better to Predict Surgical Correction of the Main Curve?Global Spine J. 2025 May;15(4):2318-2325. doi: 10.1177/21925682241299339. Epub 2025 Jan 10. Global Spine J. 2025. PMID: 39797418 Free PMC article.
-
Predicting Surgical and Non-surgical Curvature Correction by Radiographic Spinal Flexibility Assessments for Patients With Adolescent Idiopathic Scoliosis: A Systematic Review and Meta-Analysis.Global Spine J. 2025 Jun;15(5):2822-2838. doi: 10.1177/21925682251319543. Epub 2025 Feb 20. Global Spine J. 2025. PMID: 39980162 Free PMC article. Review.
-
Comparison of slot-scanning standing, supine, and fulcrum radiographs for assessment of curve flexibility in adolescent idiopathic scoliosis: a pilot study.Spine Deform. 2021 Sep;9(5):1355-1362. doi: 10.1007/s43390-021-00349-9. Epub 2021 May 6. Spine Deform. 2021. PMID: 33959933
-
Predictability of Coronal Curve Flexibility in Postoperative Curve Correction in Adolescent Idiopathic Scoliosis: The Effect of the Sagittal Profile.Global Spine J. 2020 May;10(3):303-311. doi: 10.1177/2192568219877862. Epub 2019 Sep 17. Global Spine J. 2020. PMID: 32313796 Free PMC article.
-
A retrospective controlled clinical study of Cobb angle distribution of the main thoracic curve in adolescent idiopathic scoliosis.Medicine (Baltimore). 2018 Jul;97(28):e11473. doi: 10.1097/MD.0000000000011473. Medicine (Baltimore). 2018. PMID: 29995807 Free PMC article.
References
-
- Barr SJ, Schuette AM, Emans JB (1997) Lumbar pedicle screws versus hooks: results in double major curves in adolescent idiopathic scoliosis. Spine 22: 1369–1379. - PubMed
-
- Cheng I, Kim Y, Gupta MC, Bridwell KH, Hurford RK, Lee SS, et al. (2005) Apical sublaminar wires versus pedicle screws—which provides better results for surgical correction of adolescent idiopathic scoliosis? Spine 30: 2104–2112. - PubMed
-
- Dobbs MB, Lenke LG, Kim YJ, Luhmann SJ, Bridwell KH (2006) Anterior/posterior spinal instrumentation versus posterior instrumentation alone for the treatment of adolescent idiopathic scoliotic curves more than 90. Spine 31: 2386–2391. - PubMed
-
- Lowenstein JE, Matsumoto H, Vitale MG, Weidenbaum M, Gomez JA, Lee FY, et al. (2007) Coronal and sagittal plane correction in adolescent idiopathic scoliosis: a comparison between all pedicle screw versus hybrid thoracic hook lumbar screw constructs. Spine 32: 448–452. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
