

Simultaneous Prediction of New Morbidity, Mortality, and Survival Without New Morbidity From Pediatric Intensive Care: A New Paradigm for Outcomes Assessment
- PMID: 25985385
- PMCID: PMC4657566
- DOI: 10.1097/CCM.0000000000001081
Simultaneous Prediction of New Morbidity, Mortality, and Survival Without New Morbidity From Pediatric Intensive Care: A New Paradigm for Outcomes Assessment
Abstract
Objectives: Assessments of care including quality assessments adjusted for physiological status should include the development of new morbidities as well as mortalities. We hypothesized that morbidity, like mortality, is associated with physiological dysfunction and could be predicted simultaneously with mortality.
Design: Prospective cohort study from December 4, 2011, to April 7, 2013.
Setting: General and cardiac/cardiovascular PICUs at seven sites.
Patients: Randomly selected PICU patients from their first PICU admission.
Interventions: None.
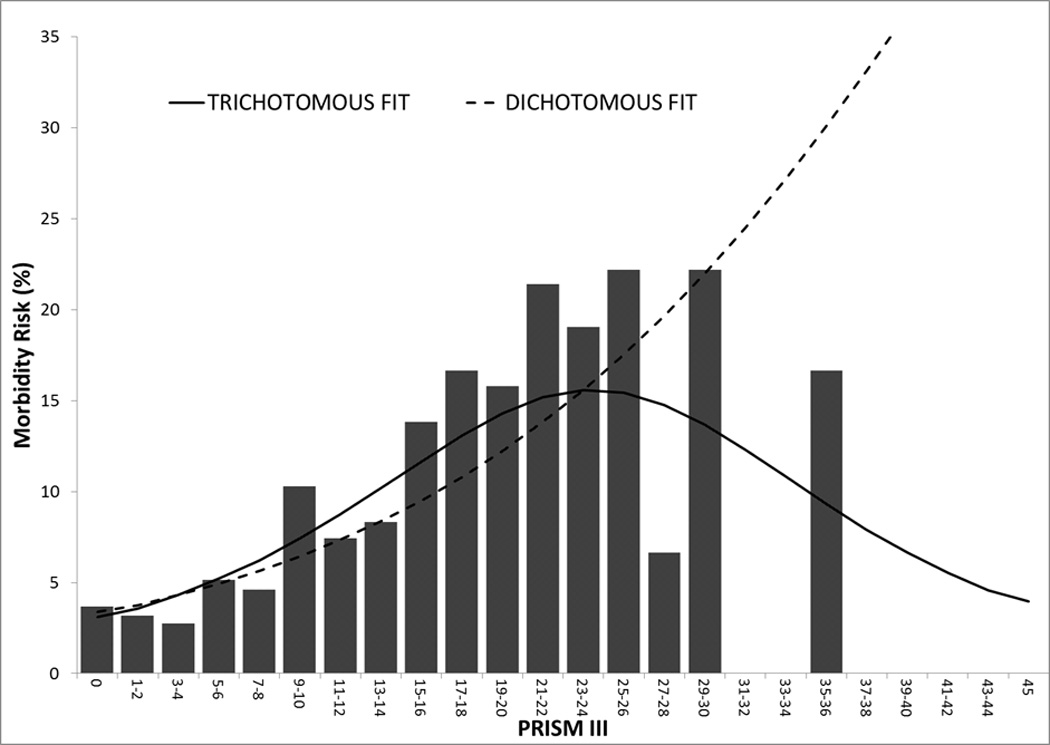
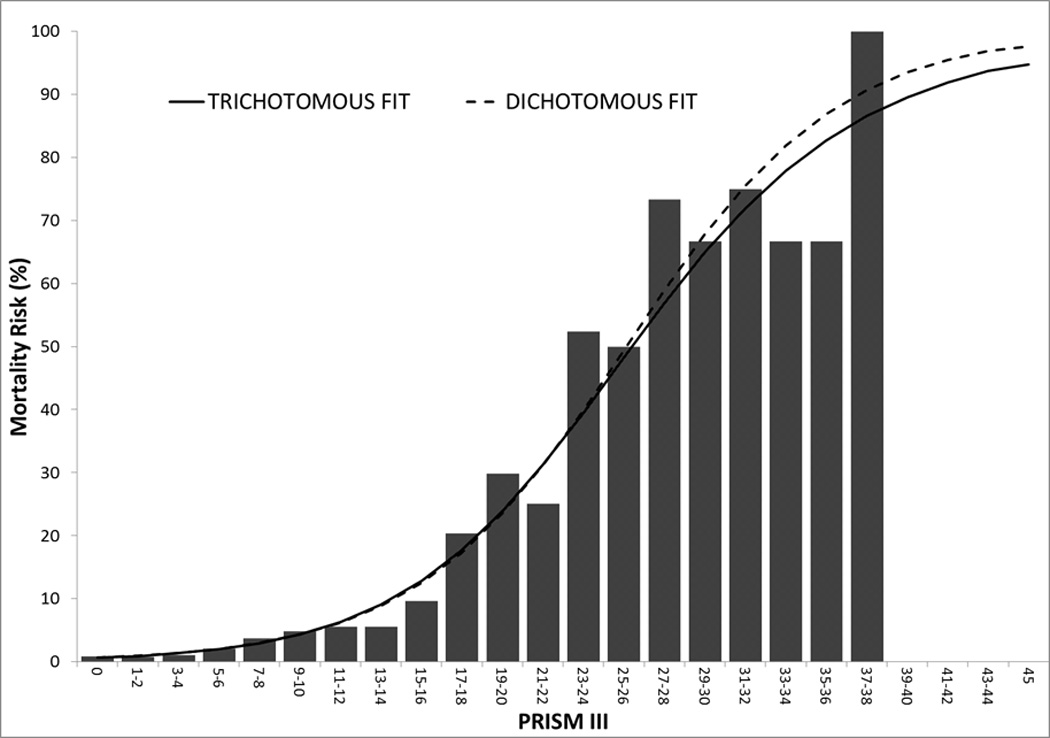
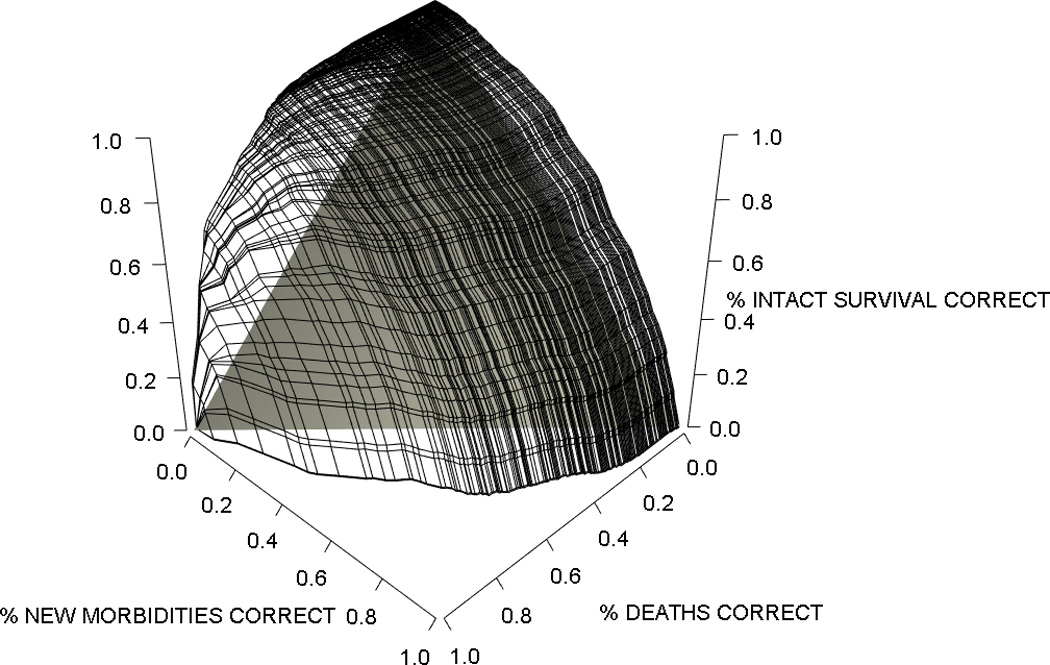
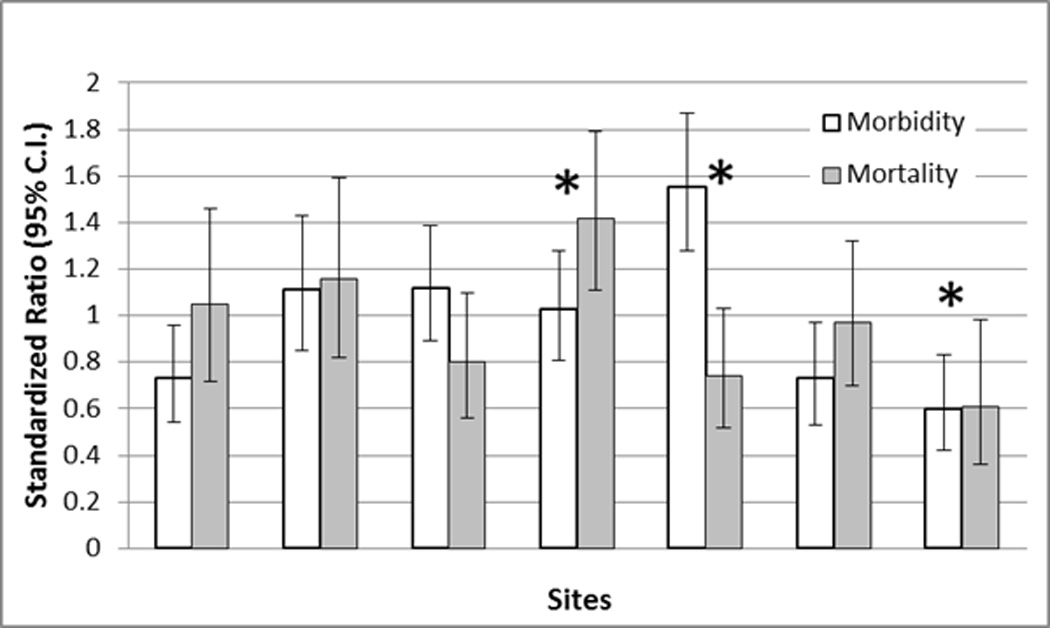
Measurements and main results: Among 10,078 admissions, the unadjusted morbidity rates (measured with the Functional Status Scale and defined as an increase of ≥ 3 from preillness to hospital discharge) were 4.6% (site range, 2.6-7.7%) and unadjusted mortality rates were 2.7% (site range, 1.3-5.0%). Morbidity and mortality were significantly (p < 0.001) associated with physiological instability (measured with the Pediatric Risk of Mortality III score) in dichotomous (survival and death) and trichotomous (survival without new morbidity, survival with new morbidity, and death) models without covariate adjustments. Morbidity risk increased with increasing Pediatric Risk of Mortality III scores and then decreased at the highest Pediatric Risk of Mortality III values as potential morbidities became mortalities. The trichotomous model with covariate adjustments included age, admission source, diagnostic factors, baseline Functional Status Scale, and the Pediatric Risk of Mortality III score. The three-level goodness-of-fit test indicated satisfactory performance for the derivation and validation sets (p > 0.20). Predictive ability assessed with the volume under the surface was 0.50 ± 0.019 (derivation) and 0.50 ± 0.034 (validation) (vs chance performance = 0.17). Site-level standardized morbidity ratios were more variable than standardized mortality ratios.
Conclusions: New morbidities were associated with physiological status and can be modeled simultaneously with mortality. Trichotomous outcome models including both morbidity and mortality based on physiological status are suitable for research studies and quality and other outcome assessments. This approach may be applicable to other assessments presently based only on mortality.
Figures
Comment in
-
Incorporating Morbidity Into PICU Quality Measures: A "TOPICC" of Critical Importance.Crit Care Med. 2015 Aug;43(8):1781-2. doi: 10.1097/CCM.0000000000001103. Crit Care Med. 2015. PMID: 26181120 No abstract available.
References
-
- Pollack MM, Ruttimann UE, Getson PR. Accurate prediction of the outcome of pediatric intensive care. A new quantitative method. N Engl J Med. 1987 Jan 15;316(3):134–139. - PubMed
-
- Knaus WA, Zimmerman JE, Wagner DP, Draper EA, Lawrence DE. APACHE-acute physiology and chronic health evaluation: a physiologically based classification system. Critical Care Medicine. 1981 Aug;9(8):591–597. - PubMed
-
- Teres D, Lemeshow S, Avrunin JS, Pastides H. Validation of the mortality prediction model for ICU patients. Critical Care Medicine. 1987 Mar;15(3):208–213. - PubMed
-
- Richardson DK, Gray JE, McCormick MC, Workman K, Goldmann DA. Score for Neonatal Acute Physiology: a physiologic severity index for neonatal intensive care. Pediatrics. 1993 Mar;91(3):617–623. - PubMed
-
- Pollack MM, Patel KM, Ruttimann UE. PRISM III: an updated Pediatric Risk of Mortality score. Critical Care Medicine. 1996 May;24(5):743–752. - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD063108/HD/NICHD NIH HHS/United States
- U01HD049934/HD/NICHD NIH HHS/United States
- U10 HD050012/HD/NICHD NIH HHS/United States
- UG1 HD050012/HD/NICHD NIH HHS/United States
- U10HD049981/HD/NICHD NIH HHS/United States
- UG1 HD049983/HD/NICHD NIH HHS/United States
- UG1 HD050096/HD/NICHD NIH HHS/United States
- U10 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049983/HD/NICHD NIH HHS/United States
- U10 HD063106/HD/NICHD NIH HHS/United States
- UG1 HD063108/HD/NICHD NIH HHS/United States
- RL1 HD107773/HD/NICHD NIH HHS/United States
- U10HD063114/HD/NICHD NIH HHS/United States
- U10HD050096/HD/NICHD NIH HHS/United States
- U10 HD063114/HD/NICHD NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
- UG1 HD049981/HD/NICHD NIH HHS/United States
- U10HD050012/HD/NICHD NIH HHS/United States
- U10 HD049981/HD/NICHD NIH HHS/United States
- U10HD063106/HD/NICHD NIH HHS/United States
- U10HD049983/HD/NICHD NIH HHS/United States
- U10HD063108/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
