

Time to First Morning Cigarette and Risk of Chronic Obstructive Pulmonary Disease: Smokers in the PLCO Cancer Screening Trial
- PMID: 25985429
- PMCID: PMC4436174
- DOI: 10.1371/journal.pone.0125973
Time to First Morning Cigarette and Risk of Chronic Obstructive Pulmonary Disease: Smokers in the PLCO Cancer Screening Trial
Abstract
Background: Time to first cigarette (TTFC) after waking is an indicator of nicotine dependence. The association between TTFC and chronic obstructive pulmonary disease (COPD), the third leading cause of death in the United States, has not yet been reported.
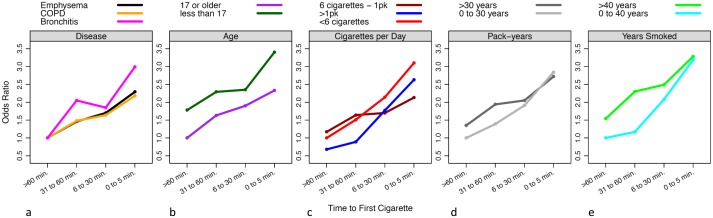
Methods: We investigated the cross-sectional association between TTFC and prevalent COPD among 6,108 current smokers in the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening Trial. COPD was defined as a self-reported diagnosis of emphysema, chronic bronchitis, or both. Current smokers in PLCO reported TTFC, the amount of time they typically waited before smoking their first cigarette of the day after waking, in four categories: ≤ 5, 6-30, 31-60, or > 60 minutes. We used logistic regression models to investigate the association between TTFC and prevalent COPD with adjustments for age, gender, race, education, and smoking (cigarettes/day, years smoked during lifetime, pack-years, age at smoking initiation), and prior lung cancer diagnosis.
Results: COPD was reported by 19% of these 6,108 smokers. Individuals with the shortest TTFC had the greatest risk of COPD; compared to those with the longest TTFC (> 60 minutes) the adjusted odds ratios (OR) and 95% confidence intervals (CI) for COPD were 1.48 (95% CI, 1.15-1.91), 1.64 (95% CI, 1.29-2.08), 2.18 (95% CI, 1.65-2.87) for those with TTFC 31-60 minutes, 6-30 minutes, and ≤ 5 minutes, respectively (P-trend < 0.0001). The association between TTFC and emphysema was similar to that for bronchitis, albeit the ORs were slightly stronger for chronic bronchitis; comparing TTFC ≤5 minutes to > 60 minutes, the adjusted OR (95% CI) was 2.29 (1.69-3.12) for emphysema and 2.99 (1.95-4.59) for chronic bronchitis.
Conclusions: Current smokers with shorter TTFC have increased risk of COPD compared to those with longer TTFC, even after comprehensive adjustment for established smoking covariates. Future epidemiologic studies, including prospective designs, should incorporate TTFC to better assess disease risk and evaluate the potential utility of TTFC as a COPD screening tool for smokers in the clinical setting.
Conflict of interest statement
Figures
Similar articles
-
Time to First Cigarette, a Proxy of Nicotine Dependence, Increases the Risk of Pulmonary Impairment, Independently of Current and Lifetime Smoking Behavior.Nicotine Tob Res. 2016 Jun;18(6):1431-9. doi: 10.1093/ntr/ntv291. Epub 2016 Jan 4. Nicotine Tob Res. 2016. PMID: 26729736
-
Time to smoke first morning cigarette and lung cancer in a case-control study.J Natl Cancer Inst. 2014 Jun 19;106(6):dju118. doi: 10.1093/jnci/dju118. Print 2014 Jun. J Natl Cancer Inst. 2014. PMID: 24948709 Free PMC article.
-
Cigarette smoking and pancreatic cancer risk: a revisit with an assessment of the nicotine dependence phenotype.Asian Pac J Cancer Prev. 2013;14(7):4409-13. doi: 10.7314/apjcp.2013.14.7.4409. Asian Pac J Cancer Prev. 2013. PMID: 23992012
-
[Smoking cessation in smokers with chronic obstructive pulmonary disease].Rev Mal Respir. 2014 Dec;31(10):937-60. doi: 10.1016/j.rmr.2014.07.001. Epub 2014 Aug 18. Rev Mal Respir. 2014. PMID: 25496790 Review. French.
-
Time to First Cigarette: A Potential Clinical Screening Tool for Nicotine Dependence.J Addict Med. 2020 Sep/Oct;14(5):409-414. doi: 10.1097/ADM.0000000000000610. J Addict Med. 2020. PMID: 31972768 Free PMC article.
Cited by
-
Association of nicotine dependence and gut microbiota: a bidirectional two-sample Mendelian randomization study.Front Immunol. 2023 Nov 7;14:1244272. doi: 10.3389/fimmu.2023.1244272. eCollection 2023. Front Immunol. 2023. PMID: 38022531 Free PMC article.
-
"Wake-and-bake" cannabis use: Predictors and cannabis-related outcomes of use shortly after waking.Drug Alcohol Depend. 2023 Jul 1;248:109937. doi: 10.1016/j.drugalcdep.2023.109937. Epub 2023 May 18. Drug Alcohol Depend. 2023. PMID: 37236059 Free PMC article.
-
CYP2A6 metabolism in the development of smoking behaviors in young adults.Addict Biol. 2018 Jan;23(1):437-447. doi: 10.1111/adb.12477. Epub 2016 Dec 29. Addict Biol. 2018. PMID: 28032407 Free PMC article.
-
Genome-wide association study across European and African American ancestries identifies a SNP in DNMT3B contributing to nicotine dependence.Mol Psychiatry. 2018 Sep;23(9):1911-1919. doi: 10.1038/mp.2017.193. Epub 2017 Oct 3. Mol Psychiatry. 2018. PMID: 28972577 Free PMC article.
-
Morning cannabis use in young adults: Associations with overall levels of use, negative consequences, and cannabis use disorder symptoms across 2.5 years.Drug Alcohol Depend. 2024 Mar 1;256:111114. doi: 10.1016/j.drugalcdep.2024.111114. Epub 2024 Feb 1. Drug Alcohol Depend. 2024. PMID: 38325066 Free PMC article.
References
-
- Centers for Disease Control and Prevention (CDC). Smoking-attributable mortality, years of potential life lost, and productivity losses—United States, 2000–2004. MMWR: Morbidity and Mortality Weekly Report. 2008;57:1226–8. Available: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5745a3.htm. - PubMed
-
- National Heart Lung and Blood Institute. Morbidity and Mortality: 2012 Chart Book on Cardiovascular, Lung, and Blood Diseases. 2012. Available from: Available: http://www.nhlbi.nih.gov/files/docs/research/2012_ChartBook_508.pdf.
-
- Kanner RE, Connett JE, Williams DE, Buist AS. Effects of randomized assignment to a smoking cessation intervention and changes in smoking habits on respiratory symptoms in smokers with early chronic obstructive pulmonary disease: the Lung Health Study. Am J Med. 1999. April;106(4):410–6. 10.1016/S0002-9343(99)00056-X - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
