

Five biopsy specimens from the proximal part of the tumor reliably determine HER2 protein expression status in gastric cancer
- PMID: 25987463
- PMCID: PMC4824804
- DOI: 10.1007/s10120-015-0502-3
Five biopsy specimens from the proximal part of the tumor reliably determine HER2 protein expression status in gastric cancer
Abstract
Background: National guidelines recommend trastuzumab for treatment of patients with metastatic HER2-positive gastric cancer (GC). There is currently no guideline indicating the number of biopsy specimens and the location from which they should be obtained to reliably determine the human epidermal growth factor receptor 2 (HER2) status in GC. The aim of this pilot study was (a) to quantify HER2-positive tumor cells in different tumor regions to assess the spatial heterogeneity of HER2 expression and (b) to establish the required number of biopsy specimens and the location from which they should be obtained within the tumor to achieve concordance between HER2 expression status in the biopsy specimens and the resection specimen.
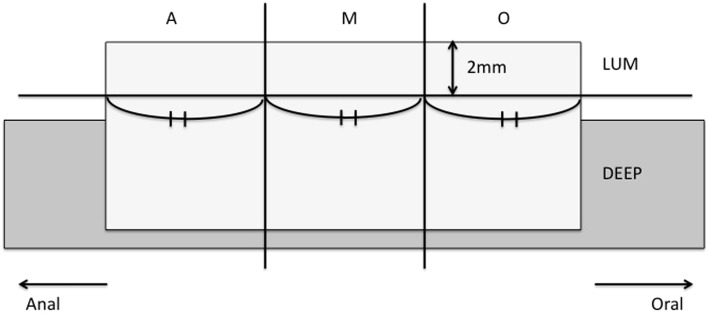
Methods: HER2 expression was quantified in six different regions of 24 HER2-positive GC and in six virtual biopsy specimens from different luminal regions. Intratumoral regional heterogeneity and concordance between HER2 status in the biopsy specimens and the resection specimen were analyzed.
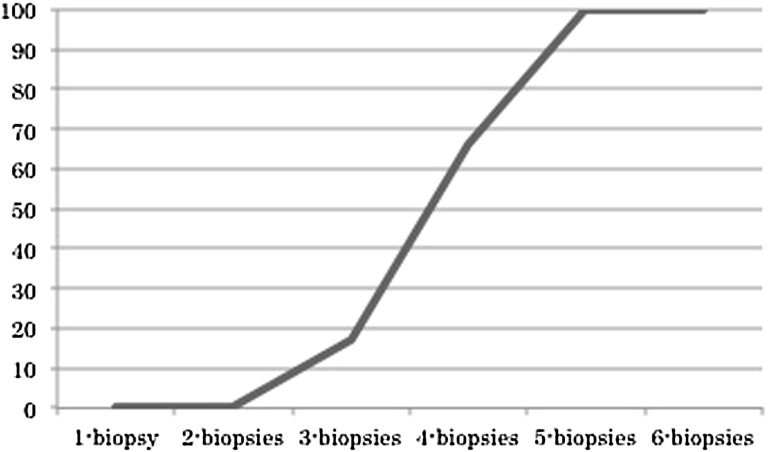
Results: HER2-positive cells were more frequent in the luminal tumor surface compared with deeper layers (p < 0.001). GCs with differentiated histological features were more commonly HER2 positive (p < 0.001). Assessment of HER2 expression status in five biopsy specimens was sufficient to achieve 100 % concordance between the biopsy specimens and the resection specimen.
Conclusions: This is the first study to suggest preferential HER2 positivity at the luminal surface in GC and to establish a minimum number of biopsy specimens needed to obtain a biopsy HER2 result which is identical to that from the whole tumor. Our study suggests that HER2 testing in five tumor-containing endoscopic biopsy specimens from the proximal (oral) part of the tumor is advisable. The results from this pilot study require validation in a prospective study.
Keywords: Gastric cancer; HER2 expression; Virtual biopsy.
Figures


References
-
- Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, et al. GLOBOCAN 2012 v1.0, cancer incidence and mortality worldwide: IARC CancerBase no. 11. Lyon: International Agency for Research on Cancer; 2013.
-
- Bang YJ, Van Cutsem E, Feyereislova A, Chung HC, Shen L, Sawaki A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376:687–697. doi: 10.1016/S0140-6736(10)61121-X. - DOI - PubMed
-
- Ajani JA, Bentrem DJ, Besh S, D’Amico TA, Das P, Denlinger C, et al. Gastric cancer, version 2.2013: featured updates to the NCCN guidelines. J Natl Compr Cancer Netw. 2013;11(5):531–546. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
