

Long-Term Treatment Outcomes of Patients Infected With Hepatitis C Virus: A Systematic Review and Meta-analysis of the Survival Benefit of Achieving a Sustained Virological Response
- PMID: 25987643
- PMCID: PMC4530725
- DOI: 10.1093/cid/civ396
Long-Term Treatment Outcomes of Patients Infected With Hepatitis C Virus: A Systematic Review and Meta-analysis of the Survival Benefit of Achieving a Sustained Virological Response
Abstract
Background: Achievement of a sustained virologic response (SVR) after treatment for Hepatitis C infection is associated with improved outcomes. This meta-analysis aimed to determine the impact of SVR on long-term mortality risk compared with nonresponders in a range of populations.
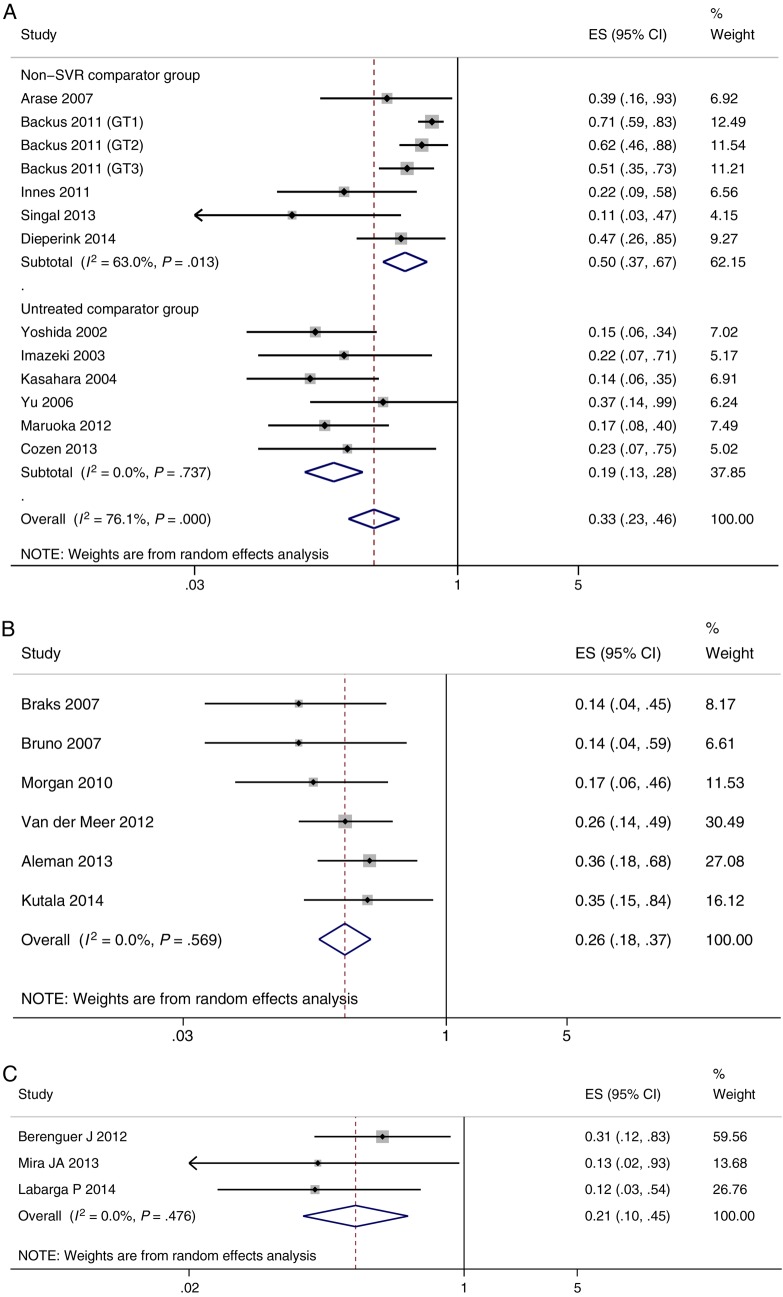
Methods: An electronic search identified all studies assessing all-cause mortality in SVR and non-SVR patients. Eligible articles were stratified into general, cirrhotic, and populations coinfected with human immunodeficiency virus. The adjusted hazard ratio (95% confidence interval [CI]) for mortality in patients achieving SVR vs non-SVR, and pooled estimates for the 5-year mortality in each group were calculated.
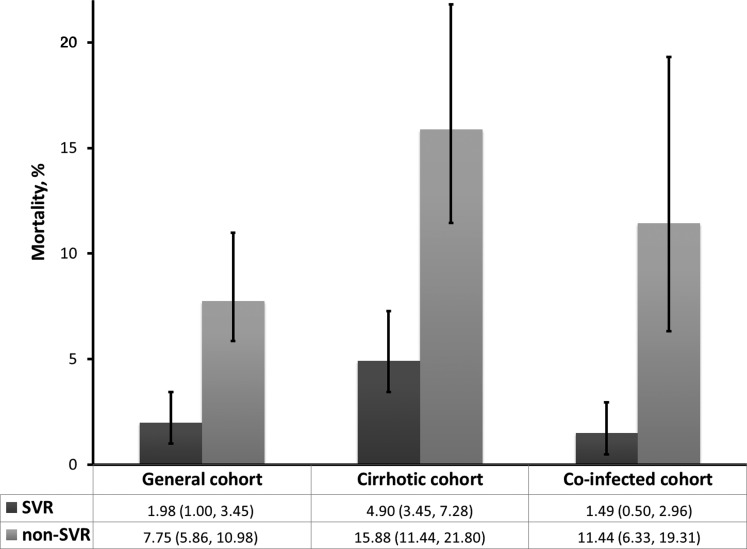
Results: 31 studies (n = 33 360) were identified as suitable for inclusion. Median follow-up time was 5.4 years (interquartile range, 4.9-7.5) across all studies. The adjusted hazard ratio of mortality for patients achieving SVR vs non-SVR was 0.50 (95% CI, .37-.67) in the general population, 0.26 (95% CI, .18-.74) in the cirrhotic group, and 0.21 (.10-.45) in the coinfected group. The pooled 5-year mortality rates were significantly lower for patients achieving SVR compared with non-SVR in all 3 populations.
Conclusions: The results suggest that there is a significant survival benefit of achieving an SVR compared with unsuccessful treatment in a range of populations infected with hepatitis C virus.
Keywords: hepatitis C; mortality; survival; sustained virologic response.
© The Author 2015. Published by Oxford University Press on behalf of the Infectious Diseases Society of America.
Figures
References
-
- Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology 2013; 57:1333–42. - PubMed
-
- Cooke G, Lemoine M, Thursz M et al. Viral hepatitis and the Global Burden of Disease: a need to regroup. J Viral Hept 2013; 20:600–1. - PubMed
-
- MSF. The diagnosis and treatment of hepatitis C: a technical landscape. Geneva, Switzerland: MSF Access Campaign, 2014.
-
- World Health Organization. Guidelines for the screening, care and treatment of persons with hepatitis C infection. Geneva, Switzerland: WHO, 2014. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
