

Multidetector computed tomography in the preoperative staging of gastric adenocarcinoma
- PMID: 25987747
- PMCID: PMC4433295
- DOI: 10.1590/0100-3984.2014.0021
Multidetector computed tomography in the preoperative staging of gastric adenocarcinoma
Abstract
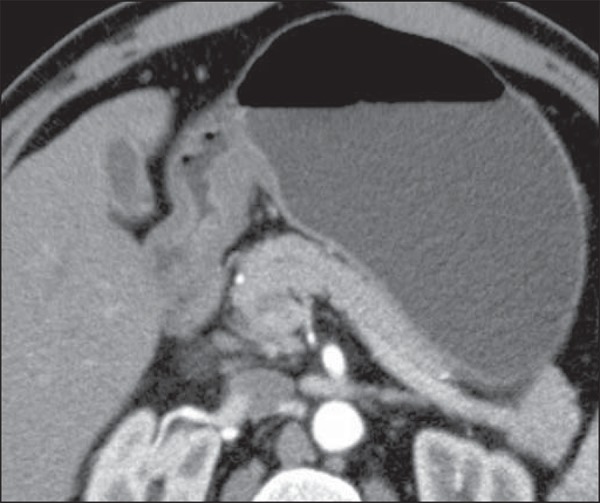
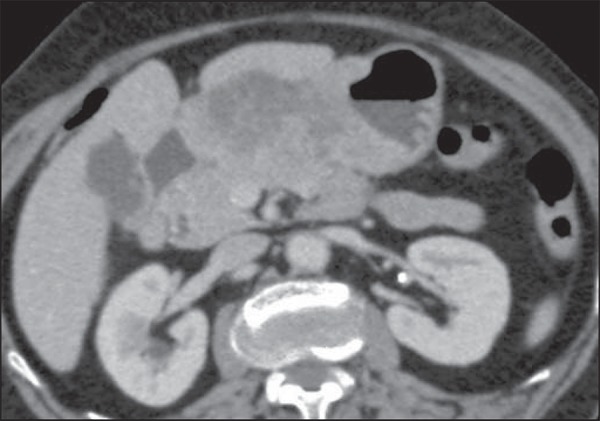
Objective: To evaluate the role of multidetector computed tomography in the preoperative investigation of tumor invasion depth and lymph node and metastatic involvement according to the TNM classification, in patients with gastric adenocarcinoma.
Materials and methods: Fifty-four patients with biopsy-confirmed gastric cancer underwent preoperative staging with 64-channel multidetector computed tomography. Two independent radiologists analyzed the images and classified the findings. Sensitivity, specificity, accuracy and overall accuracy were calculated for each observer. The interobserver agreement was also evaluated.
Results: The accuracy in the classification of categories T ranged from 74% to 96% for observer 1 and from 80% to 92% for observer 2. The overall accuracy was 70% for both observers. The weighted kappa index was 0.75, consistent with a significant interobserver agreement. The accuracy in the classification of lymph node involvement (category N) ranged from 55% to 79% for observer 1 and from 73% to 82% for observer 2. The evaluation of metastatic involvement showed an overall accuracy of 89.6% for both observers.
Conclusion: 64-channel multidetector computed tomography demonstrated clinically relevant accuracy in the preoperative staging of gastric adenocarcinoma as regards invasion depth (T category) and metastatic involvement (M category).
Objetivo: Avaliar a tomografia computadorizada com múltiplas fileiras de detectores na análise pré-operatória da profundidade de invasão tumoral, acometimento linfonodal e metastático, de acordo com a classificação TNM, em pacientes com adenocarcinoma gástrico.
Materiais e métodos: Cinquenta e quatro pacientes com câncer gástrico foram submetido a estadiamento pré-operatório com tomografia computadorizada de 64 canais de detectores. Dois radiologistas analisaram, independentemente, as imagens e classificaram os achados. A sensibilidade, especificidade, acurácia e acurácia global para cada avaliador foram calculadas. A concordância interobservador também foi avaliada.
Resultados: A acurácia na classificação das categorias T variou entre 74% e 96% para o observador 1 e entre 80% e 92% para o observador 2. A acurácia global foi 70% para ambos os observadores. O kappa ponderado foi 0,75, consistente com uma concordância interobservador substancial. A acurácia na classificação do acometimento linfonodal (categoria N) variou entre 55% e 79% para o observador 1 e entre 73% e 82% para o observador 2. A avaliação do acometimento metastático mostrou acurácia global de 89,6% para ambos os observadores.
Conclusão: A tomografia computadorizada com 64 canais de detectores demonstrou acurácia clinicamente relevante no estadiamento pré-operatório do adenocarcinoma gástrico em relação à profundidade de invasão e acometimento metastático.
Keywords: Computed tomography; Gastric cancer; Staging.
Figures


References
-
- Ferlay J, Soerjomataram I, Ervik M, et al. Globocan 2012 v1.0, Cancer incidence and mortality worldwide: IARC CancerBase No. 11. Lyon France: International Agency for Research on Cancer; 2013. [[cited 2013 Dec 12]]. [Internet] Available from: http://globocan.iarc.fr.
-
- Thrumurthy SG, Chaudry MA, Hochhauser D, et al. The diagnosis and management of gastric cancer. BMJ. 2013;347:f6367. - PubMed
-
- Edge S, Byrd DR, Compton CC, et al. AJCC cancer staging handbook. 7th ed. New York: Springer-Verlag; 2010.
-
- Lee MH, Choi D, Park MJ, et al. Gastric cancer: imaging and staging with MDCT based on the 7th AJCC guidelines. Abdom Imaging. 2012;37:531–540. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources