

Prevalence of amyloid PET positivity in dementia syndromes: a meta-analysis
- PMID: 25988463
- PMCID: PMC4517678
- DOI: 10.1001/jama.2015.4669
Prevalence of amyloid PET positivity in dementia syndromes: a meta-analysis
Abstract
Importance: Amyloid-β positron emission tomography (PET) imaging allows in vivo detection of fibrillar plaques, a core neuropathological feature of Alzheimer disease (AD). Its diagnostic utility is still unclear because amyloid plaques also occur in patients with non-AD dementia.
Objective: To use individual participant data meta-analysis to estimate the prevalence of amyloid positivity on PET in a wide variety of dementia syndromes.
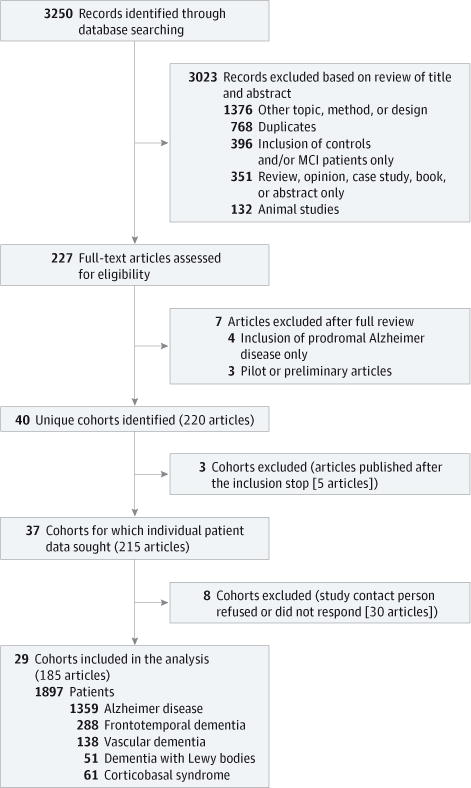
Data sources: The MEDLINE and Web of Science databases were searched from January 2004 to April 2015 for amyloid PET studies.
Study selection: Case reports and studies on neurological or psychiatric diseases other than dementia were excluded. Corresponding authors of eligible cohorts were invited to provide individual participant data.
Data extraction and synthesis: Data were provided for 1359 participants with clinically diagnosed AD and 538 participants with non-AD dementia. The reference groups were 1849 healthy control participants (based on amyloid PET) and an independent sample of 1369 AD participants (based on autopsy).
Main outcomes and measures: Estimated prevalence of positive amyloid PET scans according to diagnosis, age, and apolipoprotein E (APOE) ε4 status, using the generalized estimating equations method.
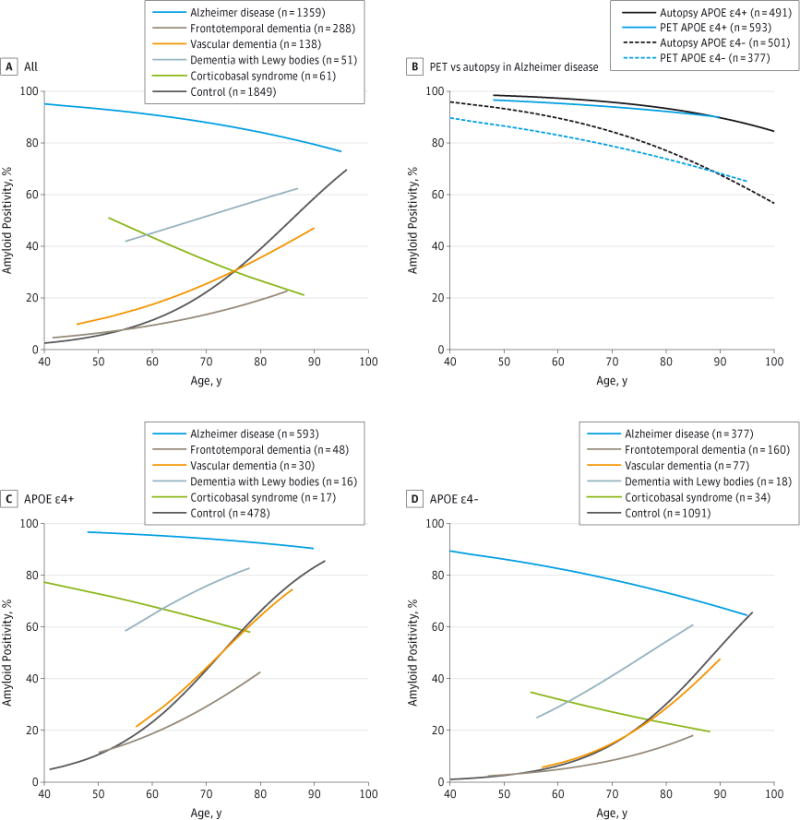
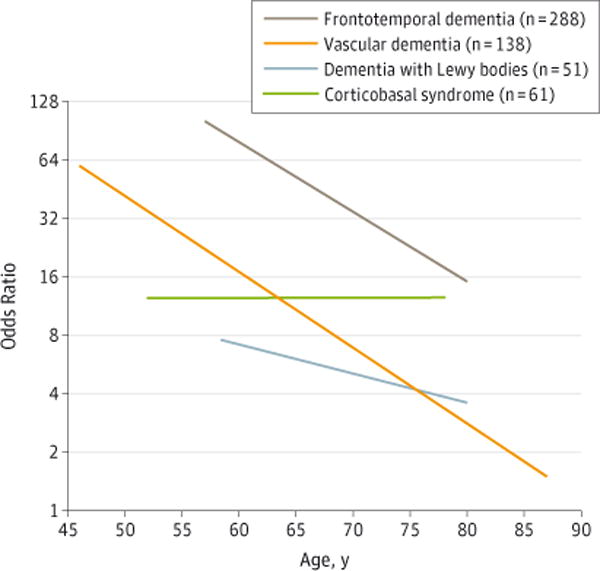
Results: The likelihood of amyloid positivity was associated with age and APOE ε4 status. In AD dementia, the prevalence of amyloid positivity decreased from age 50 to 90 years in APOE ε4 noncarriers (86% [95% CI, 73%-94%] at 50 years to 68% [95% CI, 57%-77%] at 90 years; n = 377) and to a lesser degree in APOE ε4 carriers (97% [95% CI, 92%-99%] at 50 years to 90% [95% CI, 83%-94%] at 90 years; n = 593; P < .01). Similar associations of age and APOE ε4 with amyloid positivity were observed in participants with AD dementia at autopsy. In most non-AD dementias, amyloid positivity increased with both age (from 60 to 80 years) and APOE ε4 carriership (dementia with Lewy bodies: carriers [n = 16], 63% [95% CI, 48%-80%] at 60 years to 83% [95% CI, 67%-92%] at 80 years; noncarriers [n = 18], 29% [95% CI, 15%-50%] at 60 years to 54% [95% CI, 30%-77%] at 80 years; frontotemporal dementia: carriers [n = 48], 19% [95% CI, 12%-28%] at 60 years to 43% [95% CI, 35%-50%] at 80 years; noncarriers [n = 160], 5% [95% CI, 3%-8%] at 60 years to 14% [95% CI, 11%-18%] at 80 years; vascular dementia: carriers [n = 30], 25% [95% CI, 9%-52%] at 60 years to 64% [95% CI, 49%-77%] at 80 years; noncarriers [n = 77], 7% [95% CI, 3%-18%] at 60 years to 29% [95% CI, 17%-43%] at 80 years.
Conclusions and relevance: Among participants with dementia, the prevalence of amyloid positivity was associated with clinical diagnosis, age, and APOE genotype. These findings indicate the potential clinical utility of amyloid imaging for differential diagnosis in early-onset dementia and to support the clinical diagnosis of participants with AD dementia and noncarrier APOE ε4 status who are older than 70 years.
Figures
Comment in
-
Defining amyloid pathology in persons with and without dementia syndromes: making the right diagnosis.JAMA. 2015 May 19;313(19):1913-4. doi: 10.1001/jama.2015.5361. JAMA. 2015. PMID: 25988459 No abstract available.
References
-
- World Health Organization. Dementia: a public health priority. 2012 http://www.who.int/mental_health/publications/dementia_report_2012/en/. Accessed April 23, 2015.
-
- Knopman DS, DeKosky ST, Cummings JL, et al. Practice parameter: diagnosis of dementia (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2001;56(9):1143–1153. - PubMed
-
- Doody RS, Thomas RG, Farlow M, et al. Alzheimer’s Disease Cooperative Study Steering Committee; Solanezumab Study Group Phase 3 trials of solanezumab for mild-to-moderate Alzheimer’s disease. N Engl J Med. 2014;370(4):311–321. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- NS075321/NS/NINDS NIH HHS/United States
- P01 AG026276/AG/NIA NIH HHS/United States
- R01 NS075321/NS/NINDS NIH HHS/United States
- P01 AG019724/AG/NIA NIH HHS/United States
- R01 AG045611/AG/NIA NIH HHS/United States
- RF1 NS075321/NS/NINDS NIH HHS/United States
- P30 AG010124/AG/NIA NIH HHS/United States
- P50 AG023501/AG/NIA NIH HHS/United States
- U01 AG024904/AG/NIA NIH HHS/United States
- P01 AD 026276/AD/ADAMHA HHS/United States
- U01 AG016976/AG/NIA NIH HHS/United States
- P01 AG003991/AG/NIA NIH HHS/United States
- P50 AG005681/AG/NIA NIH HHS/United States
- UL1RR024992/RR/NCRR NIH HHS/United States
- UL1 RR024992/RR/NCRR NIH HHS/United States
- CAPMC/ CIHR/Canada
- R01 AG032306/AG/NIA NIH HHS/United States
- P01 AD 003991/AD/ADAMHA HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
