

Lateralization of mesial temporal lobe epilepsy with chronic ambulatory electrocorticography
- PMID: 25988840
- PMCID: PMC4676303
- DOI: 10.1111/epi.13010
Lateralization of mesial temporal lobe epilepsy with chronic ambulatory electrocorticography
Abstract
Objective: Patients with suspected mesial temporal lobe (MTL) epilepsy typically undergo inpatient video-electroencephalography (EEG) monitoring with scalp and/or intracranial electrodes for 1 to 2 weeks to localize and lateralize the seizure focus or foci. Chronic ambulatory electrocorticography (ECoG) in patients with MTL epilepsy may provide additional information about seizure lateralization. This analysis describes data obtained from chronic ambulatory ECoG in patients with suspected bilateral MTL epilepsy in order to assess the time required to determine the seizure lateralization and whether this information could influence treatment decisions.
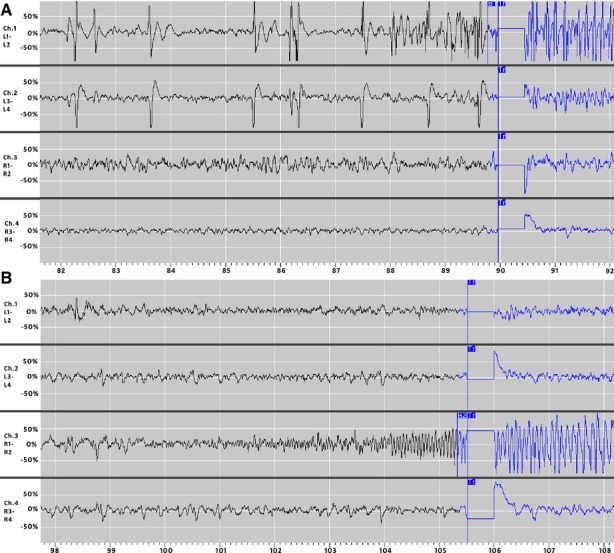
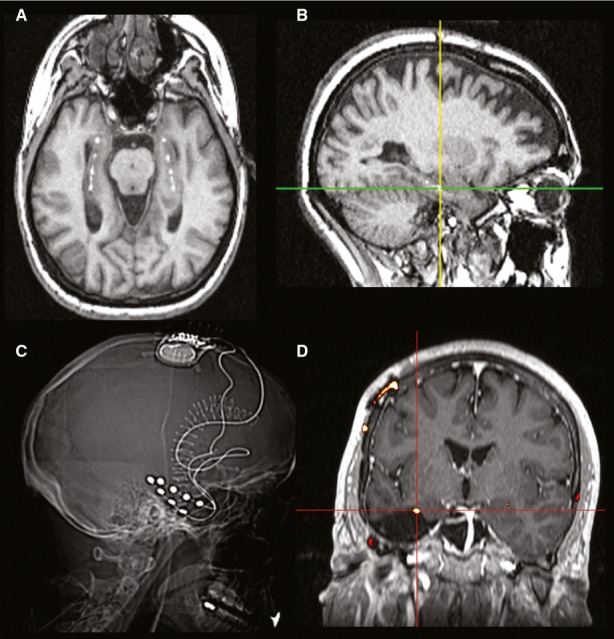
Methods: Ambulatory ECoG was reviewed in patients with suspected bilateral MTL epilepsy who were among a larger cohort with intractable epilepsy participating in a randomized controlled trial of responsive neurostimulation. Subjects were implanted with bilateral MTL leads and a cranially implanted neurostimulator programmed to detect abnormal interictal and ictal ECoG activity. ECoG data stored by the neurostimulator were reviewed to determine the lateralization of electrographic seizures and the interval of time until independent bilateral MTL electrographic seizures were recorded.
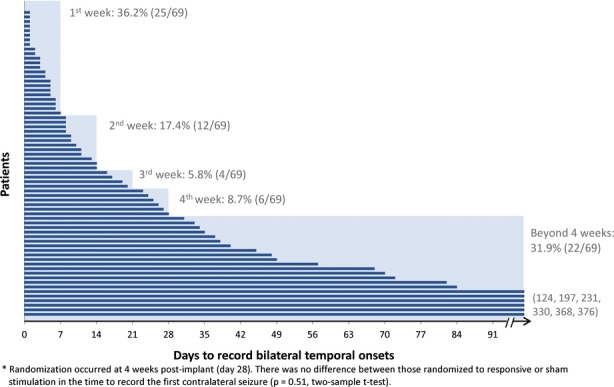
Results: Eighty-two subjects were implanted with bilateral MTL leads and followed for 4.7 years on average (median 4.9 years). Independent bilateral MTL electrographic seizures were recorded in 84%. The average time to record bilateral electrographic seizures in the ambulatory setting was 41.6 days (median 13 days, range 0-376 days). Sixteen percent had only unilateral electrographic seizures after an average of 4.6 years of recording.
Significance: About one third of the subjects implanted with bilateral MTL electrodes required >1 month of chronic ambulatory ECoG before the first contralateral MTL electrographic seizure was recorded. Some patients with suspected bilateral MTL seizures had only unilateral electrographic seizures. Chronic ambulatory ECoG in patients with suspected bilateral MTL seizures provides data in a naturalistic setting, may complement data from inpatient video-EEG monitoring, and can contribute to treatment decisions.
Keywords: Ambulatory EEG; EEG monitoring; Electrocorticography; Intracranial EEG; Localization; Responsive stimulation.
© 2015 Neuropace, Inc. Epilepsia published by Wiley Periodicals on behalf of International League Against Epilepsy.
Figures
References
-
- Engel J, Jr, Wiebe S, French J, et al. Practice parameter: temporal lobe and localized neocortical resections for epilepsy: report of the Quality Standards Subcommittee of the American Academy of Neurology, in association with the American Epilepsy Society and the American Association of Neurological Surgeons. Neurology. 2003;60:538–547. - PubMed
-
- Sum JM, Morrell MJ. Predictive value of the first ictal recording in determining localization of the epileptogenic region by scalp/sphenoidal EEG. Epilepsia. 1995;36:1033–1040. - PubMed
-
- Morrell MJ. Responsive cortical stimulation for the treatment of medically intractable partial epilepsy. Neurology. 2011;77:1295–1304. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
