

Fully automated targeting using nonrigid image registration matches accuracy and exceeds precision of best manual approaches to subthalamic deep brain stimulation targeting in Parkinson disease
- PMID: 25988929
- PMCID: PMC4438781
- DOI: 10.1227/NEU.0000000000000714
Fully automated targeting using nonrigid image registration matches accuracy and exceeds precision of best manual approaches to subthalamic deep brain stimulation targeting in Parkinson disease
Abstract
Background: Finding the optimal location for the implantation of the electrode in deep brain stimulation (DBS) surgery is crucial for maximizing the therapeutic benefit to the patient. Such targeting is challenging for several reasons, including anatomic variability between patients as well as the lack of consensus about the location of the optimal target.
Objective: To compare the performance of popular manual targeting methods against a fully automatic nonrigid image registration-based approach.
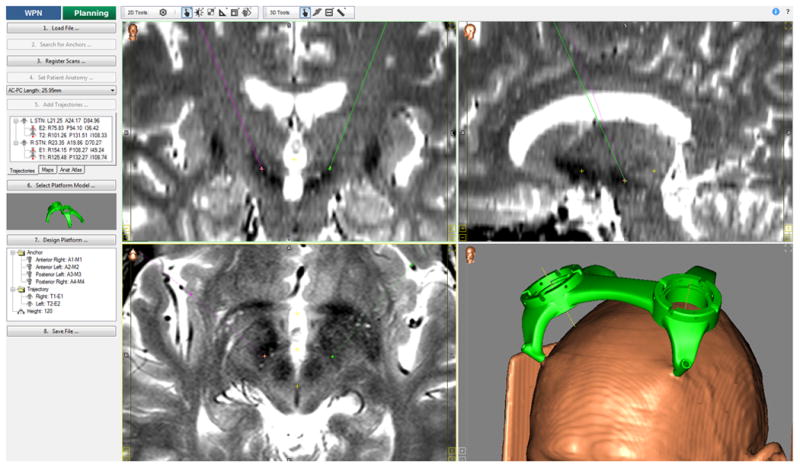
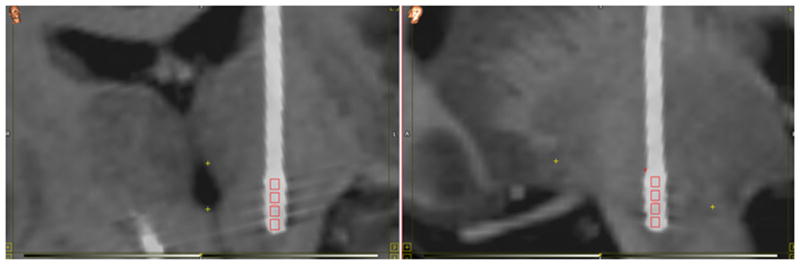
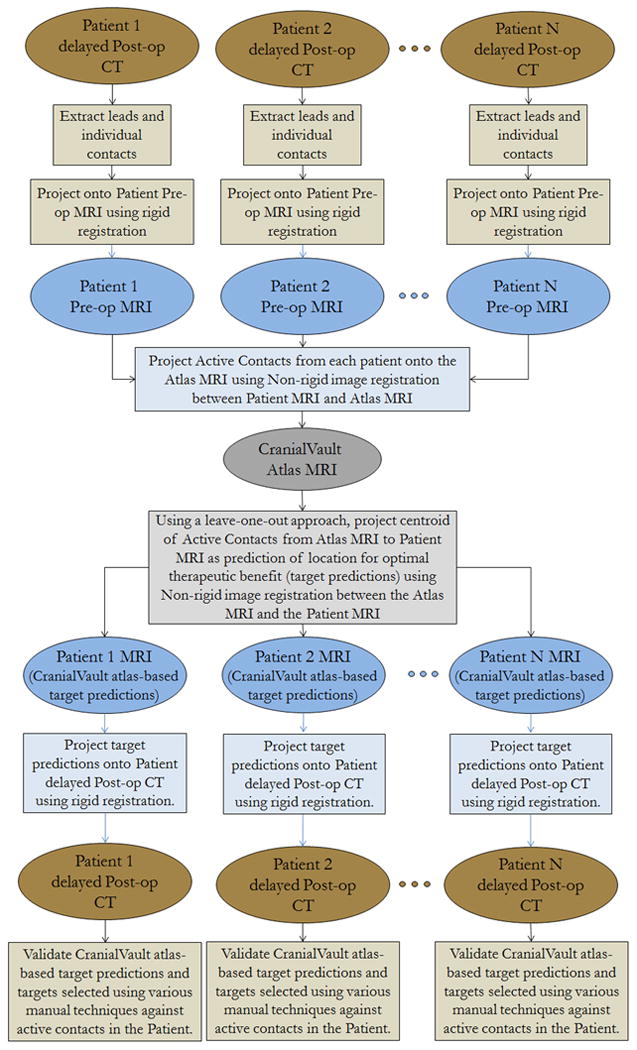
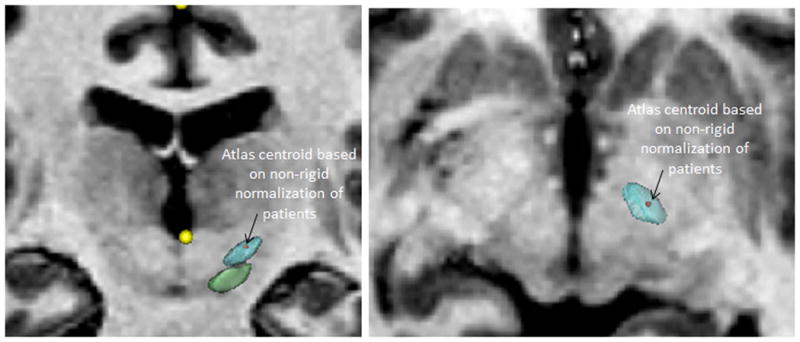
Methods: In 71 Parkinson disease subthalamic nucleus (STN)-DBS implantations, an experienced functional neurosurgeon selected the target manually using 3 different approaches: indirect targeting using standard stereotactic coordinates, direct targeting based on the patient magnetic resonance imaging, and indirect targeting relative to the red nucleus. Targets were also automatically predicted by using a leave-one-out approach to populate the CranialVault atlas with the use of nonrigid image registration. The different targeting methods were compared against the location of the final active contact, determined through iterative clinical programming in each individual patient.
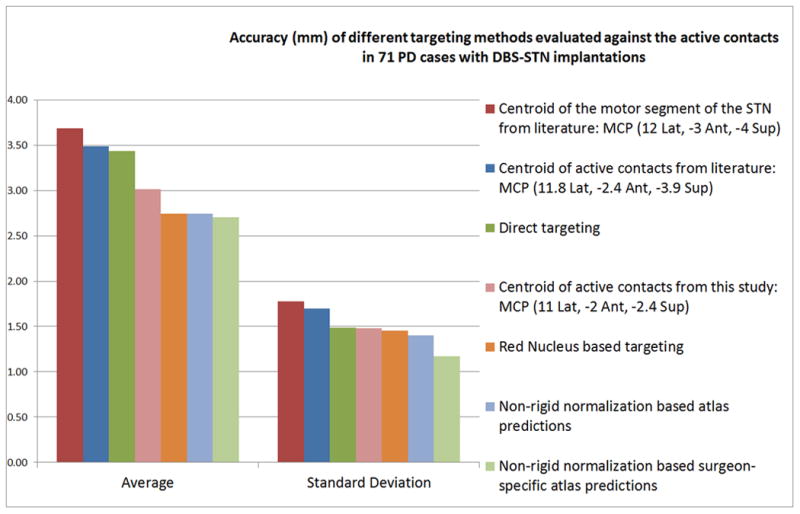
Results: Targeting by using standard stereotactic coordinates corresponding to the center of the motor territory of the STN had the largest targeting error (3.69 mm), followed by direct targeting (3.44 mm), average stereotactic coordinates of active contacts from this study (3.02 mm), red nucleus-based targeting (2.75 mm), and nonrigid image registration-based automatic predictions using the CranialVault atlas (2.70 mm). The CranialVault atlas method had statistically smaller variance than all manual approaches.
Conclusion: Fully automatic targeting based on nonrigid image registration with the use of the CranialVault atlas is as accurate and more precise than popular manual methods for STN-DBS.
Conflict of interest statement
Figures
References
-
- Binder DK, R GM, Starr PA. Risk factors for hemorrhage during microelectrode-guided deep brain stimulator implantation for movement disorders. Neurosurgery. 2005;56(4):722–732. - PubMed
-
- Xiaowu H, Xiufeng J, Xiaoping Z, Bin H, et al. Risks of intracranial hemorrhage in patients with Parkinson's disease receiving deep brain stimulation and ablation. Parkinsonism & related disorders. 2010;16(2):96–100. - PubMed
-
- Starr PA, Christine CW, Theodosopoulos PV, et al. Implantation of deep brain stimulators into the subthalamic nucleus: technical approach and magnetic resonance imaging-verified lead locations. J Neurosurg. 2002 Aug;97(2):370–387. - PubMed
-
- Benabid AL, Krack PP, Benazzouz A, Limousin P, Koudsie A, Pollak P. Deep brain stimulation of the subthalamic nucleus for Parkinson's disease: methodologic aspects and clinical criteria. Neurology. 2000;55(12 Suppl 6):S40–44. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
