

Patient Preferences and Surrogate Decision Making in Neuroscience Intensive Care Units
- PMID: 25990137
- PMCID: PMC4816524
- DOI: 10.1007/s12028-015-0149-2
Patient Preferences and Surrogate Decision Making in Neuroscience Intensive Care Units
Abstract
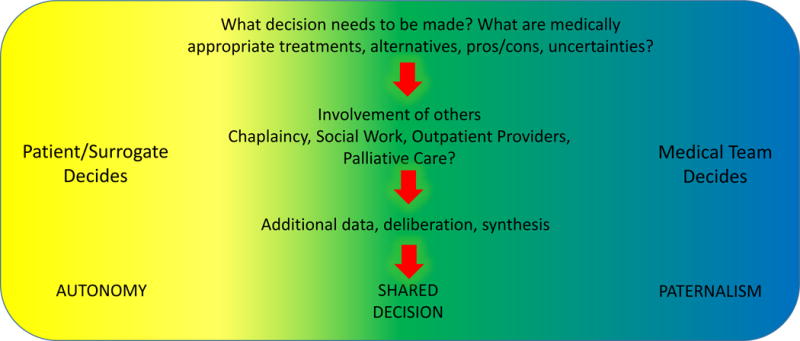
In the neuroscience intensive care unit (NICU), most patients lack the capacity to make their own preferences known. This fact leads to situations where surrogate decision makers must fill the role of the patient in terms of making preference-based treatment decisions, oftentimes in challenging situations where prognosis is uncertain. The neurointensivist has a large responsibility and role to play in this shared decision-making process. This review covers how NICU patient preferences are determined through existing advance care documentation or surrogate decision makers and how the optimum roles of the physician and surrogate decision maker are addressed. We outline the process of reaching a shared decision between family and care team and describe a practice for conducting optimum family meetings based on studies of ICU families in crisis. We review challenges in the decision-making process between surrogate decision makers and medical teams in neurocritical care settings, as well as methods to ameliorate conflicts. Ultimately, the goal of shared decision making is to increase knowledge amongst surrogates and care providers, decrease decisional conflict, promote realistic expectations and preference-centered treatment strategies, and lift the emotional burden on families of neurocritical care patients.
Conflict of interest statement
Xuemei Cai, Jennifer Robinson, Susanne Muehlschlegel, Kevin N. Sheth, and Robert G. Holloway declare that they have no conflicts of interest. Douglas B. White has no relevant conflicts of interest and receives research support from NIH 1R01AG045176-01 and 1R01NR014663. Liana Fraenkel receives research support from the NIH 5K24AR060231-02, 5P60AR047782, and the VA Health Services Research IIR. David Y. Hwang has received an American Brain Foundation Practice Research Training Fellowship.
Figures
References
-
-
Patient Self Determination Act. Pub. L. No. 101–508, ss 4206(a), 4751(m), 104 Stat. 1388–116, 1990.
-
-
- Starr P. The Social Transformation of American Medicine. 1982 Basic Books New York
-
- Brudney D. Choosing for another: beyond autonomy and best interests. The Hastings Center report. 2009;39:31–7. - PubMed
-
- Smedira NG, Evans BH, Grais LS, et al. Withholding and withdrawal of life support from the critically ill. The New England journal of medicine. 1990;322:309–15. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
