

Cost-effectiveness and public health benefit of secondary cardiovascular disease prevention from improved adherence using a polypill in the UK
- PMID: 25991449
- PMCID: PMC4452741
- DOI: 10.1136/bmjopen-2014-007111
Cost-effectiveness and public health benefit of secondary cardiovascular disease prevention from improved adherence using a polypill in the UK
Abstract
Objective: To evaluate the public health and economic benefits of adherence to a fixed-dose combination polypill for the secondary prevention of cardiovascular (CV) events in adults with a history of myocardial infarction (MI) in the UK.
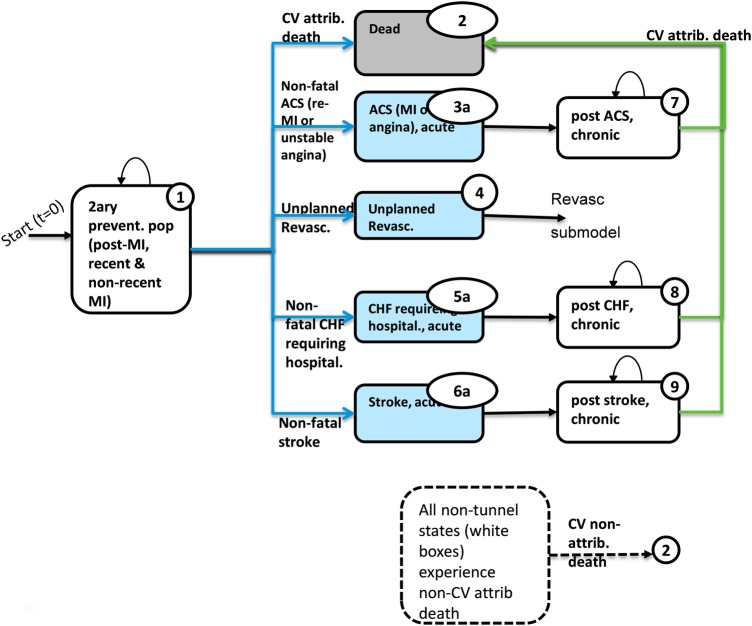
Design: Markov-model-based cost-effectiveness analysis, informed by systematic reviews, which identified efficacy, utilities and adherence data inputs.
Setting: General practice in the UK.
Participants: Patients with a mean age of 64.7 years, most of whom are men with a recent or non-recent diagnosis of MI and for whom secondary preventive medication is indicated and well tolerated.
Intervention: Fixed-dose combination polypill (100 mg aspirin, 20 mg atorvastatin and 2.5, 5, or 10 mg ramipril) compared with multiple monotherapy.
Primary and secondary outcome measures: CV events prevented per 1000 patients; cost per life-year gained; and cost per quality-adjusted life-year (QALY) gained.
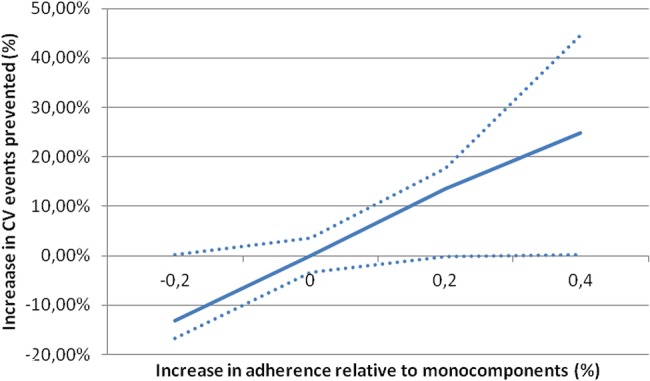
Results: The model estimates that for each 10% increase in adherence, an additional 6.7% fatal and non-fatal CV events can be prevented. In the base case, over 10 years, the polypill would improve adherence by ∼20% and thereby prevent 47 of 323 (15%) fatal and non-fatal CV events per 1000 patients compared with multiple monotherapy, with an incremental cost-effectiveness ratio (ICER) of £8200 per QALY gained. Probabilistic sensitivity analyses for the base-case assumptions showed an 81.5% chance of the polypill being cost-effective at a willingness-to-pay threshold of £20,000 per QALY gained compared with multiple monotherapy. In scenario analyses that varied structural assumptions, ICERs ranged between cost saving and £21,430 per QALY gained.
Conclusions: Assuming that some 450,000 adults are at risk of MI, a 10 percentage point uptake of the polypill could prevent 3260 CV events and 590 CV deaths over a decade.The polypill appears to be a cost-effective strategy to prevent fatal and non-fatal CV events in the UK.
Keywords: CARDIOLOGY; PREVENTIVE MEDICINE.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- National Institute for Health and Care Excellence (NICE). MI-secondary prevention: secondary prevention in primary and secondary care for patients following a myocardial infarction [CG172]. London, UK: National Institute for Health and Care Excellence, 2013. http://guidance.nice.org.uk/CG172 (accessed Jun 2014).
-
- Lafeber M, Spiering W, van der Graaf Y et al. The combined use of aspirin, a statin, and blood pressure-lowering agents (polypill components) and the risk of vascular morbidity and mortality in patients with coronary artery disease. Am Heart J 2013;166:282–89.e1. 10.1016/j.ahj.2013.04.011 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources