

Improving Clinical Outcomes in Patients With Methicillin-Sensitive Staphylococcus aureus Bacteremia and Reported Penicillin Allergy
- PMID: 25991471
- PMCID: PMC4542891
- DOI: 10.1093/cid/civ394
Improving Clinical Outcomes in Patients With Methicillin-Sensitive Staphylococcus aureus Bacteremia and Reported Penicillin Allergy
Abstract
Background: Methicillin-sensitive Staphylococcus aureus (MSSA) bacteremia is a morbid infection. First-line MSSA therapies (nafcillin, oxacillin, cefazolin) are generally avoided in the 10% of patients reporting penicillin (PCN) allergy, but most of these patients are not truly allergic. We used a decision tree with sensitivity analyses to determine the optimal evaluation and treatment for patients with MSSA bacteremia and reported PCN allergy.
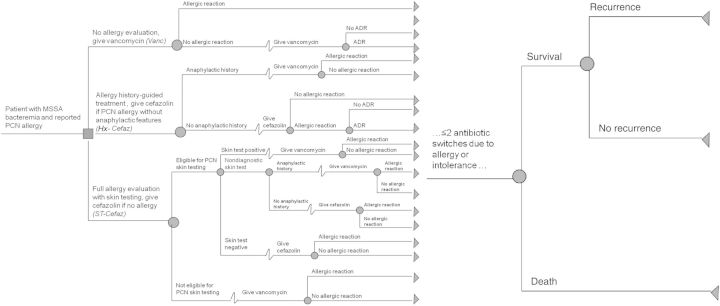
Methods: Our model simulates 3 strategies: (1) no allergy evaluation, give vancomycin (Vanc); (2) allergy history-guided treatment: if history excludes anaphylactic features, give cefazolin (Hx-Cefaz); and (3) complete allergy evaluation with history-appropriate PCN skin testing: if skin test negative, give cefazolin (ST-Cefaz). Model outcomes included 12-week MSSA cure, recurrence, and death; allergic reactions including major, minor, and potentially iatrogenic; and adverse drug reactions.
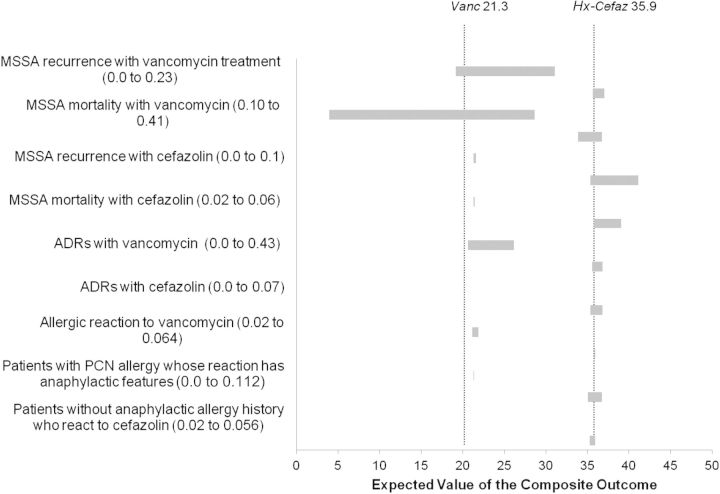
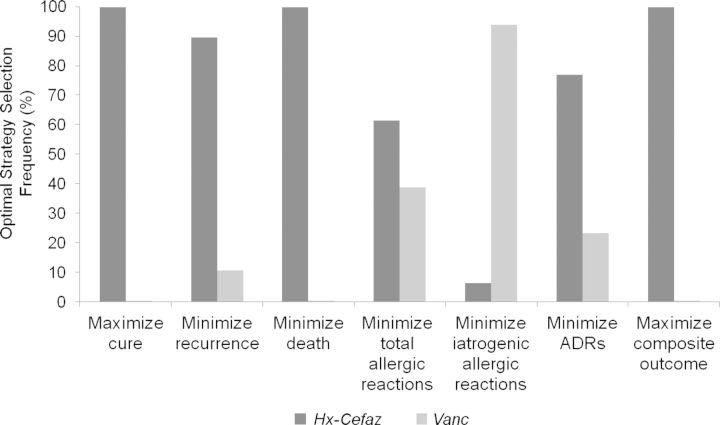
Results: Vanc results in the fewest patients achieving MSSA cure and the highest rate of recurrence (67.3%/14.8% vs 83.4%/9.3% for Hx-Cefaz and 84.5%/8.9% for ST-Cefaz) as well as the greatest frequency of allergic reactions (3.0% vs 2.4% for Hx-Cefaz and 1.7% for ST-Cefaz) and highest rates of adverse drug reactions (5.2% vs 4.6% for Hx-Cefaz and 4.7% for ST-Cefaz). Even in a "best case for Vanc" scenario, Vanc yields the poorest outcomes. ST-Cefaz is preferred to Hx-Cefaz although sensitive to input variations.
Conclusions: Patients with MSSA bacteremia and a reported PCN allergy should have the allergy addressed for optimal treatment. Full allergy evaluation with skin testing seems to be preferred, although more data are needed.
Keywords: Staphylococcus aureus; allergy; decision analysis; penicillin; vancomycin.
© The Author 2015. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Reed SD, Friedman JY, Engemann JJ, et al. Costs and outcomes among hemodialysis-dependent patients with methicillin-resistant or methicillin-susceptible Staphylococcus aureus bacteremia. Infec Control Hosp Epidemiol 2005; 26:175–83. - PubMed
-
- Cosgrove SE, Sakoulas G, Perencevich EN, Schwaber MJ, Karchmer AW, Carmeli Y. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: a meta-analysis. Clin Infect Dis 2003; 39:53–9. - PubMed
-
- Fowler VG, Sexton DJ. Clinical approach to Staphylococcus aureus bacteremia in adults. In: UpToDate, Baron EL, ed. Waltham, MA: UpToDate, 2013. Accessed 27 May 2015.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
