

Chronic abdominal pain secondary to mesenteric panniculitis treated successfully with endoscopic ultrasonography-guided celiac plexus block: A case report
- PMID: 25992196
- PMCID: PMC4436925
- DOI: 10.4253/wjge.v7.i5.563
Chronic abdominal pain secondary to mesenteric panniculitis treated successfully with endoscopic ultrasonography-guided celiac plexus block: A case report
Abstract
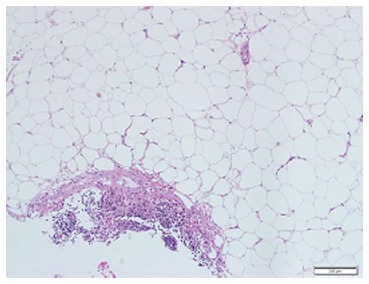
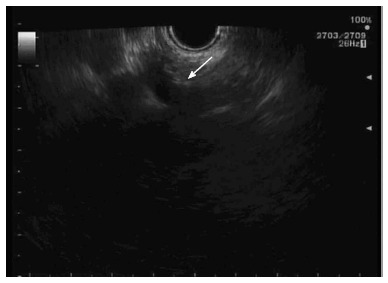
Mesenteric panniculitis is a chronic illness that is characterized by fibrosing inflammation of the mesenteries that can lead to intractable abdominal pain. Pain control is a crucial component of the management plan. Most patients will improve with oral corticosteroids treatment, however, some patients will require a trial of other immunosuppressive agents, and a minority of patients will continue to have refractory disease. Endoscopic ultrasound guided celiac plexus block is used frequently to control abdominal pain in patients with pancreatic pathology. To our knowledge there are no case reports describing its use in mesenteric panniculitis patients with refractory abdominal pain.
Keywords: Abdominal pain; Celiac plexus; Endoscopic-ultrasound; Mesenteric panniculitis.
Figures

Similar articles
-
Endoscopic ultrasound-guided celiac plexus block for managing abdominal pain associated with chronic pancreatitis: a prospective single center experience.Am J Gastroenterol. 2001 Feb;96(2):409-16. doi: 10.1111/j.1572-0241.2001.03551.x. Am J Gastroenterol. 2001. PMID: 11232683
-
A prospective randomized comparison of endoscopic ultrasound- and computed tomography-guided celiac plexus block for managing chronic pancreatitis pain.Am J Gastroenterol. 1999 Apr;94(4):900-5. doi: 10.1111/j.1572-0241.1999.01042.x. Am J Gastroenterol. 1999. PMID: 10201454 Clinical Trial.
-
Bedside ultrasound-guided celiac plexus neurolysis with bilateral paramedian needle entry technique can be an effective pain control technique in advanced upper abdominal cancer pain.J Palliat Med. 2008 Nov;11(9):1195-9. doi: 10.1089/jpm.2008.0082. J Palliat Med. 2008. PMID: 19021480
-
Efficacy of endoscopic ultrasound-guided celiac plexus block and celiac plexus neurolysis for managing abdominal pain associated with chronic pancreatitis and pancreatic cancer.J Clin Gastroenterol. 2010 Feb;44(2):127-34. doi: 10.1097/MCG.0b013e3181bb854d. J Clin Gastroenterol. 2010. PMID: 19826273 Review.
-
Celiac Plexus Block and Neurolysis: A Review.Gastrointest Endosc Clin N Am. 2018 Oct;28(4):579-586. doi: 10.1016/j.giec.2018.06.004. Epub 2018 Aug 3. Gastrointest Endosc Clin N Am. 2018. PMID: 30241645 Review.
Cited by
-
Mesenteric Panniculitis with Raised Alanine Transaminase Levels: A Rare Case Report from Pakistan.Cureus. 2019 Dec 18;11(12):e6411. doi: 10.7759/cureus.6411. Cureus. 2019. PMID: 31970040 Free PMC article.
-
A meta-analysis on the efficacy of endoscopic ultrasonography for treatment of pancreatic cancer.Clinics (Sao Paulo). 2024 Mar 28;79:100348. doi: 10.1016/j.clinsp.2024.100348. eCollection 2024. Clinics (Sao Paulo). 2024. PMID: 38552386 Free PMC article.
References
-
- Jura V. Sulla mesenterite retrattile sclerosante. Policlinico (sezprat) 1924;31:575–581.
-
- Aach RD, Kahn LI, Frech RS. Obstruction of the small intestine due to retractile mesenteritis. Gastroenterology. 1968;54:594–598. - PubMed
-
- Piessen G, Mariette C, Triboulet JP. Mesenteric panniculitis. Ann Chir. 2006;131:85–90. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
