

Sepsis outcomes in patients receiving statins prior to hospitalization for sepsis: comparison of in-hospital mortality rates between patients who received atorvastatin and those who received simvastatin
- PMID: 25992302
- PMCID: PMC4430500
- DOI: 10.1186/s13613-015-0049-9
Sepsis outcomes in patients receiving statins prior to hospitalization for sepsis: comparison of in-hospital mortality rates between patients who received atorvastatin and those who received simvastatin
Abstract
Background: The purpose of this study is to compare the in-hospital mortality rates between septic patients receiving statins and those that did not prior to developing sepsis. We compared subgroups receiving atorvastatin and simvastatin because these two drugs differ in their pharmacologic properties.
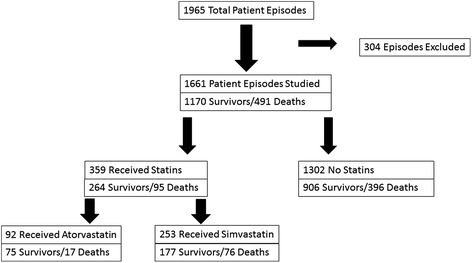
Methods: This study was a retrospective analysis of patients selected from an institutional data base of patients hospitalized with sepsis. The study patients were drawn from a data base of 1,961 hospitalized patients with sepsis and included patients who met selection criteria and who were studied for HMG-CoA reductase inhibitor (statin) use both prior to and during hospitalization. The in-hospital mortality rates of patients receiving statins and those that did not prior to developing sepsis were compared. In-hospital mortality rates of patient subgroups receiving atorvastatin and simvastatin were also compared. A multivariable analysis was conducted with in-hospital mortality as the outcome variable and with multiple risk factors to include atorvastatin and simvastatin use.
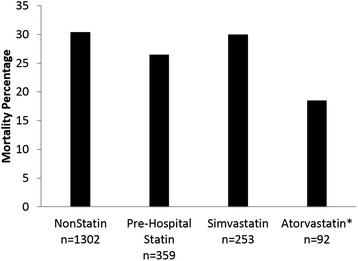
Results: The mortality rate for 359 patients receiving statins prior to hospitalization for sepsis was not significantly different than that for 1,302 patients who did not receive pre-hospital statins (26.5% versus 30.4%, p > 0.05). The mortality rate for 92 patients who had received atorvastatin prior to hospitalization was significantly less than that of 253 patients who received simvastatin (18.5% versus 30.0%, p = 0.032). The use of atorvastatin prior to sepsis was independently associated with lower in-hospital mortality in a multivariable analysis of sepsis risk factors (p = 0.021, OR = 0.455). Patients who received atorvastatin prior to hospitalization for sepsis and had statins continued in hospital had a very low mortality rate that was significantly less than that of those patients who never received statins (15.7% versus 30.8%, p = 0.007).
Conclusions: Pre-hospital atorvastatin use was associated with improved in-hospital mortality in septic patients when compared with pre-hospital simvastatin use and was independently associated with an improved outcome when compared to other sepsis risk factors. The effect of statins in patients with sepsis may be different for individual statins.
Keywords: Atorvastatin; Critical illness; HMG-CoA reductase inhibitors; Inflammation; Mortality; Sepsis.
Figures
References
-
- Hall JH, Williams SN, DeFrances CJ, Golosinskiy A. Inpatient care for septicemia or sepsis: a challenge for patients and hospitals. NCHS Data Brief 2011; No. 62. Available at: http://www.cdc.gov/nchs/data/databriefs/db62.htm. Accessed December 2, 2014. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
