

Trial of short-course antimicrobial therapy for intraabdominal infection
- PMID: 25992746
- PMCID: PMC4469182
- DOI: 10.1056/NEJMoa1411162
Trial of short-course antimicrobial therapy for intraabdominal infection
Erratum in
-
Trial of Short-Course Antimicrobial Therapy for Intraabdominal Infection.N Engl J Med. 2018 Feb 15;378(7):686. doi: 10.1056/NEJMx180006. Epub 2018 Jan 25. N Engl J Med. 2018. PMID: 29370580 No abstract available.
Abstract
Background: The successful treatment of intraabdominal infection requires a combination of anatomical source control and antibiotics. The appropriate duration of antimicrobial therapy remains unclear.
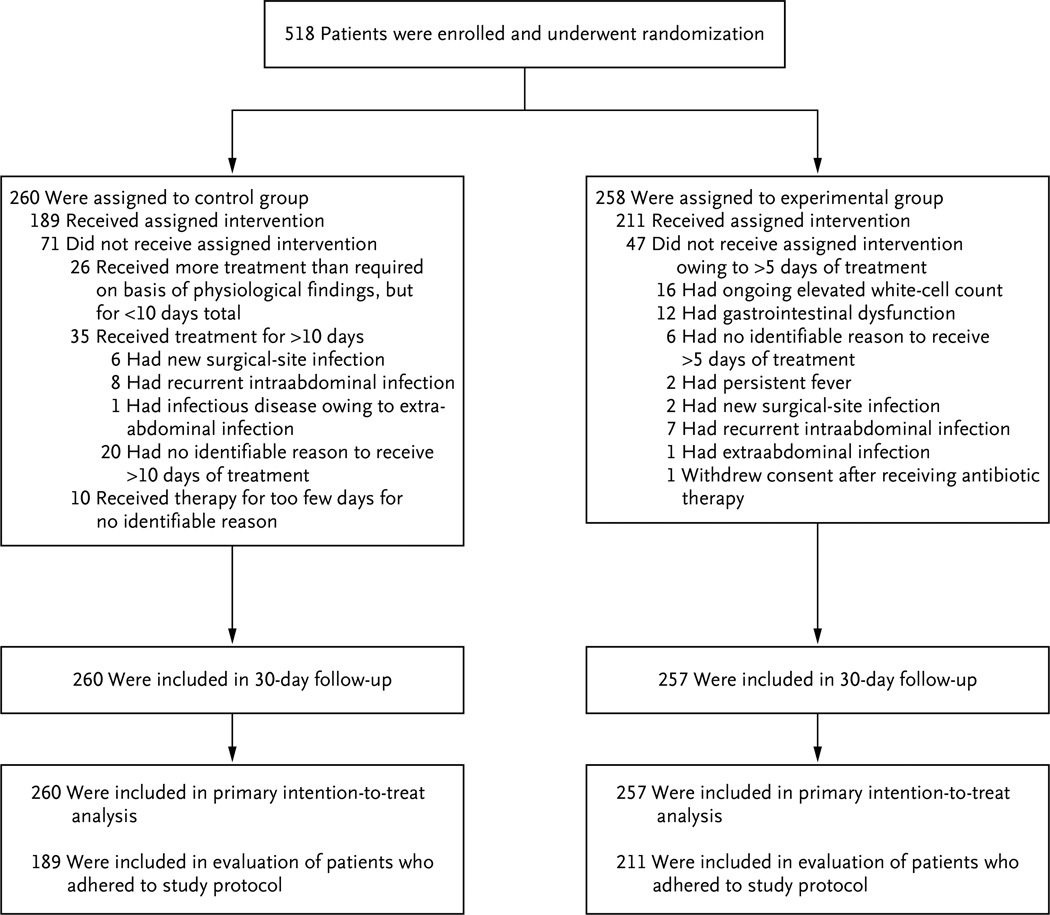
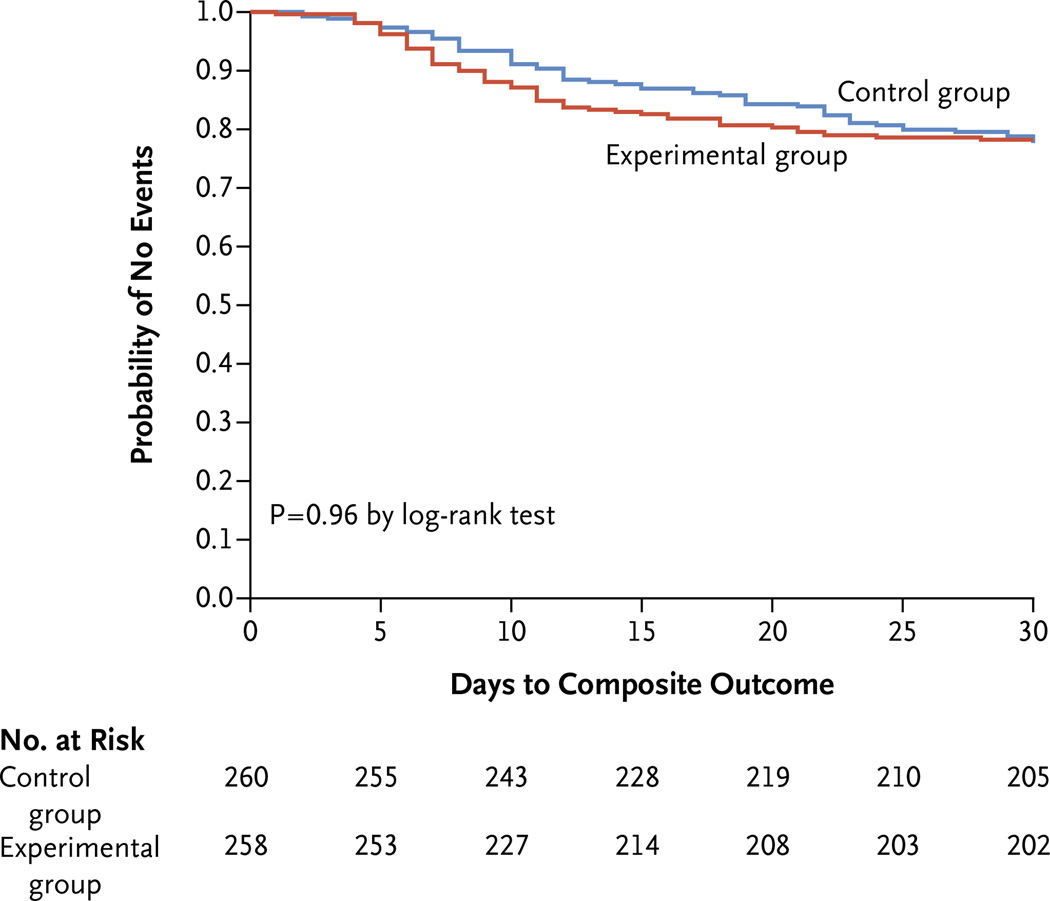
Methods: We randomly assigned 518 patients with complicated intraabdominal infection and adequate source control to receive antibiotics until 2 days after the resolution of fever, leukocytosis, and ileus, with a maximum of 10 days of therapy (control group), or to receive a fixed course of antibiotics (experimental group) for 4±1 calendar days. The primary outcome was a composite of surgical-site infection, recurrent intraabdominal infection, or death within 30 days after the index source-control procedure, according to treatment group. Secondary outcomes included the duration of therapy and rates of subsequent infections.
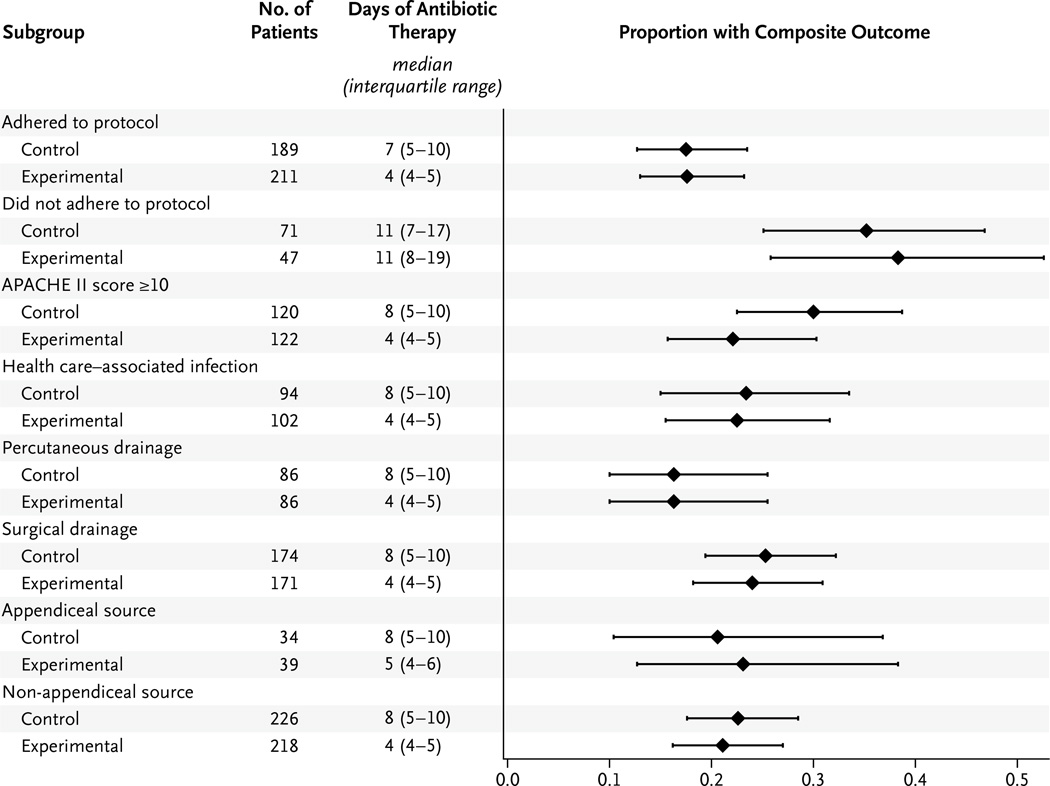
Results: Surgical-site infection, recurrent intraabdominal infection, or death occurred in 56 of 257 patients in the experimental group (21.8%), as compared with 58 of 260 patients in the control group (22.3%) (absolute difference, -0.5 percentage point; 95% confidence interval [CI], -7.0 to 8.0; P=0.92). The median duration of antibiotic therapy was 4.0 days (interquartile range, 4.0 to 5.0) in the experimental group, as compared with 8.0 days (interquartile range, 5.0 to 10.0) in the control group (absolute difference, -4.0 days; 95% CI, -4.7 to -3.3; P<0.001). No significant between-group differences were found in the individual rates of the components of the primary outcome or in other secondary outcomes.
Conclusions: In patients with intraabdominal infections who had undergone an adequate source-control procedure, the outcomes after fixed-duration antibiotic therapy (approximately 4 days) were similar to those after a longer course of antibiotics (approximately 8 days) that extended until after the resolution of physiological abnormalities. (Funded by the National Institutes of Health; STOP-IT ClinicalTrials.gov number, NCT00657566.).
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Antibiotics for abdominal sepsis.N Engl J Med. 2015 May 21;372(21):2062-3. doi: 10.1056/NEJMe1503936. N Engl J Med. 2015. PMID: 25992751 No abstract available.
-
Short-course antimicrobial therapy may be clinically similar to a longer course for complicated intra-abdominal infections.Evid Based Med. 2015 Oct;20(5):182-3. doi: 10.1136/ebmed-2015-110243. Epub 2015 Aug 20. Evid Based Med. 2015. PMID: 26294787 No abstract available.
-
[Can the duration of antibiotic therapy be reduced to 4 days in intra-abdominal infections?].Rev Prat. 2015 Jun;65(6):763. Rev Prat. 2015. PMID: 26298895 French. No abstract available.
-
Short-Course Antimicrobial Therapy for Intraabdominal Infection.N Engl J Med. 2015 Oct 15;373(16):1578. doi: 10.1056/NEJMc1508694. N Engl J Med. 2015. PMID: 26466002 Free PMC article.
-
Short-Course Antimicrobial Therapy for Intraabdominal Infection.N Engl J Med. 2015 Oct 15;373(16):1577. doi: 10.1056/NEJMc1508694. N Engl J Med. 2015. PMID: 26466003 No abstract available.
-
Short-Course Antimicrobial Therapy for Intraabdominal Infection.N Engl J Med. 2015 Oct 15;373(16):1577-8. doi: 10.1056/NEJMc1508694. N Engl J Med. 2015. PMID: 26466004 No abstract available.
-
ACP Journal Club. After source control in intraabdominal infections, 4-day and longer-duration antibiotics did not differ at 30-days.Ann Intern Med. 2015 Oct 20;163(8):JC6. doi: 10.7326/ACPJC-2015-163-8-006. Ann Intern Med. 2015. PMID: 26502143 No abstract available.
References
-
- DeFrances CJ, Cullen KA, Kozak LJ. National Hospital Discharge Survey: 2005 annual summary with detailed diagnosis and procedure data. Vital Health Stat 13. 2007;165:1–209. - PubMed
-
- Inui T, Haridas M, Claridge JA, Malangoni MA. Mortality for intra-abdominal infection is associated with intrinsic risk factors rather than the source of infection. Surgery. 2009;146:654–661. - PubMed
-
- Christou NV, Barie PS, Dellinger EP, Waymack JP, Stone HH. Surgical Infection Society intra-abdominal infection study: prospective evaluation of management techniques and outcome. Arch Surg. 1993;128:193–198. - PubMed