

Intraoperative tight glucose control using hyperinsulinemic normoglycemia increases delirium after cardiac surgery
- PMID: 25992877
- PMCID: PMC4440226
- DOI: 10.1097/ALN.0000000000000669
Intraoperative tight glucose control using hyperinsulinemic normoglycemia increases delirium after cardiac surgery
Abstract
Background: Postoperative delirium is common in patients recovering from cardiac surgery. Tight glucose control has been shown to reduce mortality and morbidity. Therefore, the authors sought to determine the effect of tight intraoperative glucose control using a hyperinsulinemic-normoglycemic clamp approach on postoperative delirium in patients undergoing cardiac surgery.
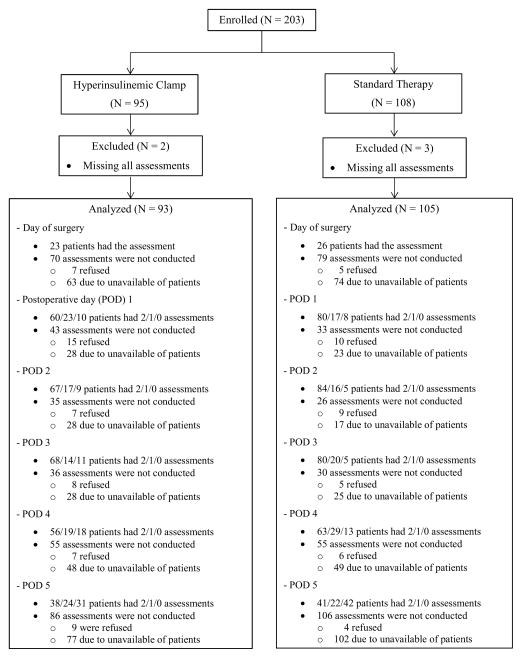
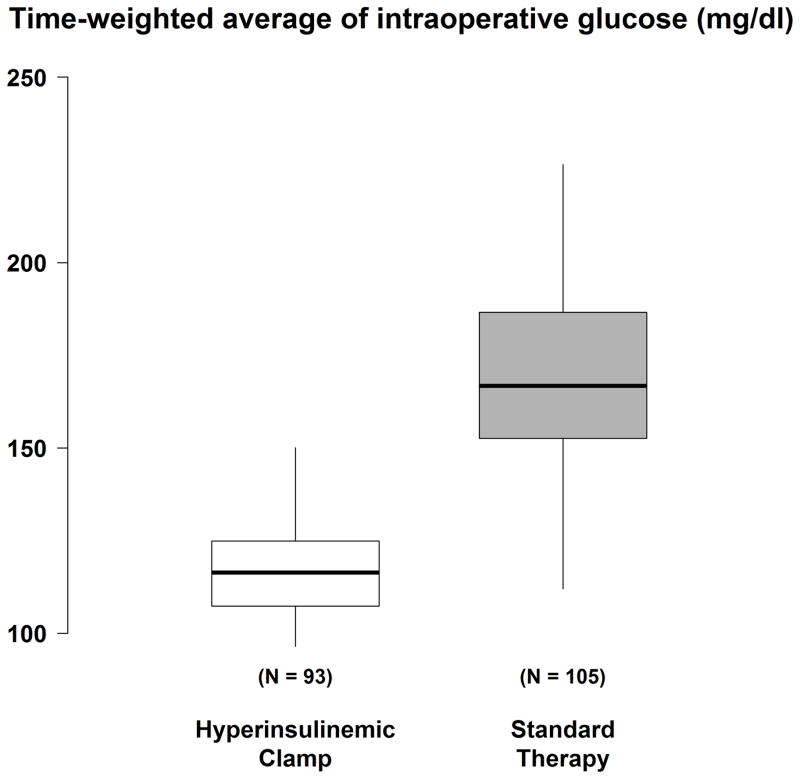
Methods: The authors enrolled 198 adult patients having cardiac surgery in this randomized, double-blind, single-center trial. Patients were randomly assigned to either tight intraoperative glucose control with a hyperinsulinemic-normoglycemic clamp (target blood glucose, 80 to 110 mg/dl) or standard therapy (conventional insulin administration with blood glucose target, <150 mg/dl). Delirium was assessed using a comprehensive delirium battery. The authors considered patients to have experienced postoperative delirium when Confusion Assessment Method testing was positive at any assessment. A positive Confusion Assessment Method was defined by the presence of features 1 (acute onset and fluctuating course) and 2 (inattention) and either 3 (disorganized thinking) or 4 (altered consciousness).
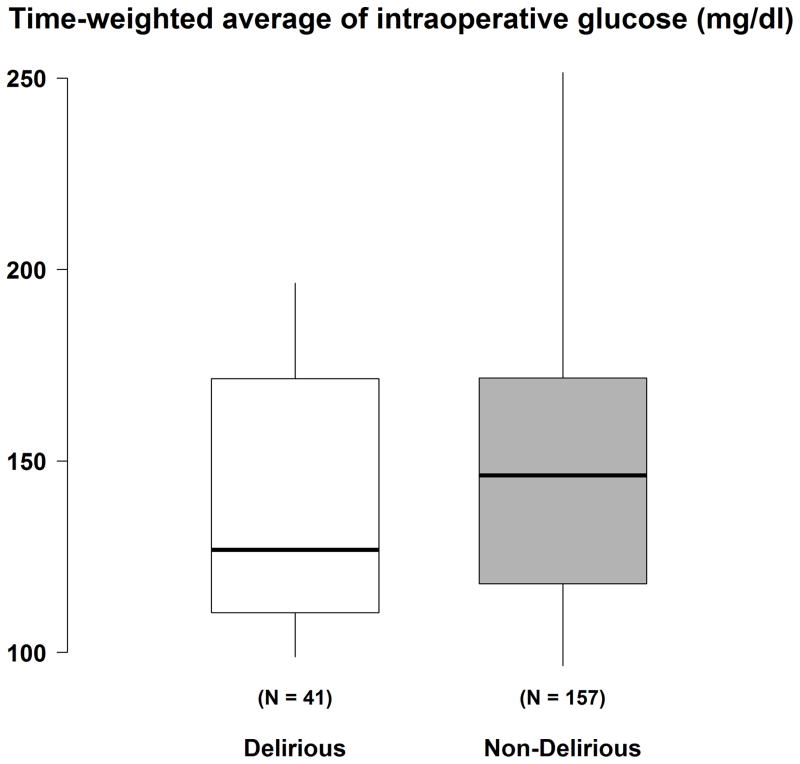
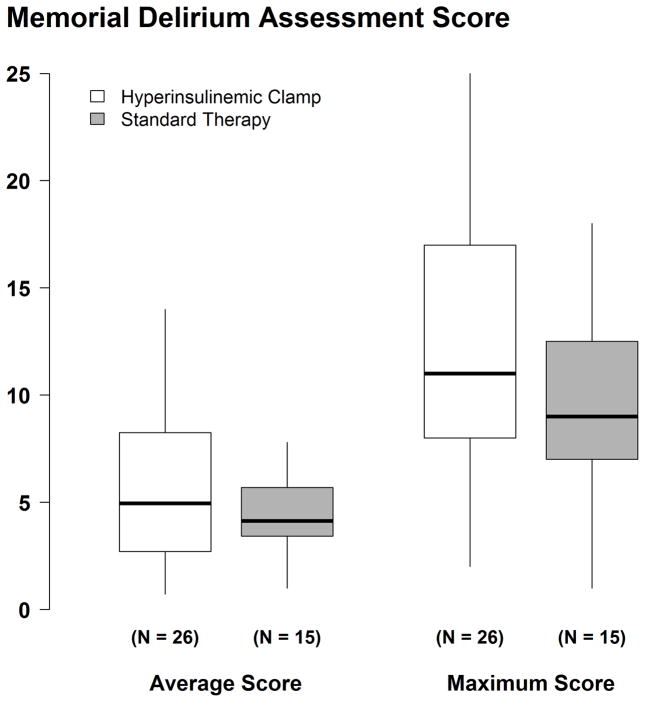
Results: Patients randomized to tight glucose control were more likely to be diagnosed as being delirious than those assigned to routine glucose control (26 of 93 vs. 15 of 105; relative risk, 1.89; 95% CI, 1.06 to 3.37; P = 0.03), after adjusting for preoperative usage of calcium channel blocker and American Society of Anesthesiologist physical status. Delirium severity, among patients with delirium, was comparable with each glucose management strategy.
Conclusion: Intraoperative hyperinsulinemic-normoglycemia augments the risk of delirium after cardiac surgery, but not its severity.
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Intraoperative Glycemic Control to Prevent Delirium after Cardiac Surgery: Steering a Course between Scylla and Charybdis.Anesthesiology. 2015 Jun;122(6):1186-8. doi: 10.1097/ALN.0000000000000670. Anesthesiology. 2015. PMID: 25844843 No abstract available.
References
-
- Ely EW, Shintani A, Truman B, Speroff T, Gordon SM, Harrell FE, Jr, Inouye SK, Bernard GR, Dittus RS. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291:1753–62. - PubMed
-
- McCusker J, Cole M, Abrahamowicz M, Primeau F, Belzile E. Delirium predicts 12-month mortality. Arch Intern Med. 2002;162:457–63. - PubMed
-
- Milbrandt EB, Deppen S, Harrison PL, Shintani AK, Speroff T, Stiles RA, Truman B, Bernard GR, Dittus RS, Ely EW. Costs associated with delirium in mechanically ventilated patients. Crit Care Med. 2004;32:955–62. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
