

Ischemia and reperfusion injury in renal transplantation: hemodynamic and immunological paradigms
- PMID: 25993079
- PMCID: PMC4946821
- DOI: 10.1590/S1679-45082015RW3161
Ischemia and reperfusion injury in renal transplantation: hemodynamic and immunological paradigms
Abstract
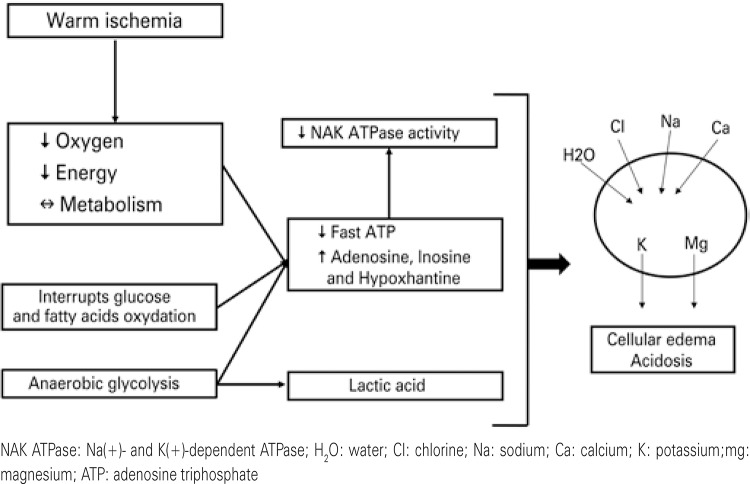
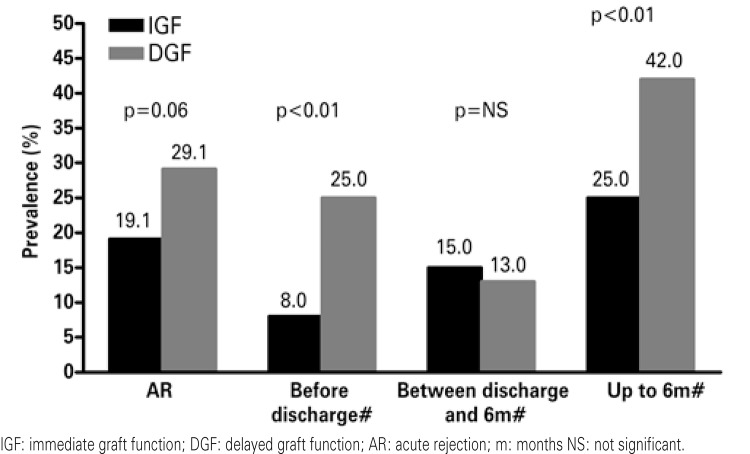
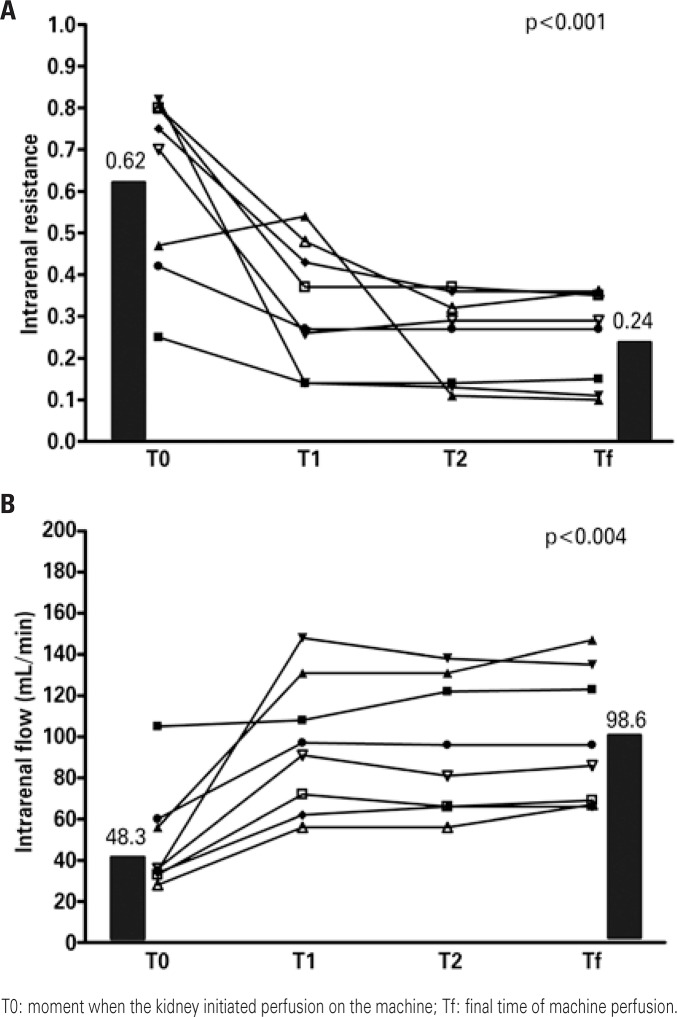
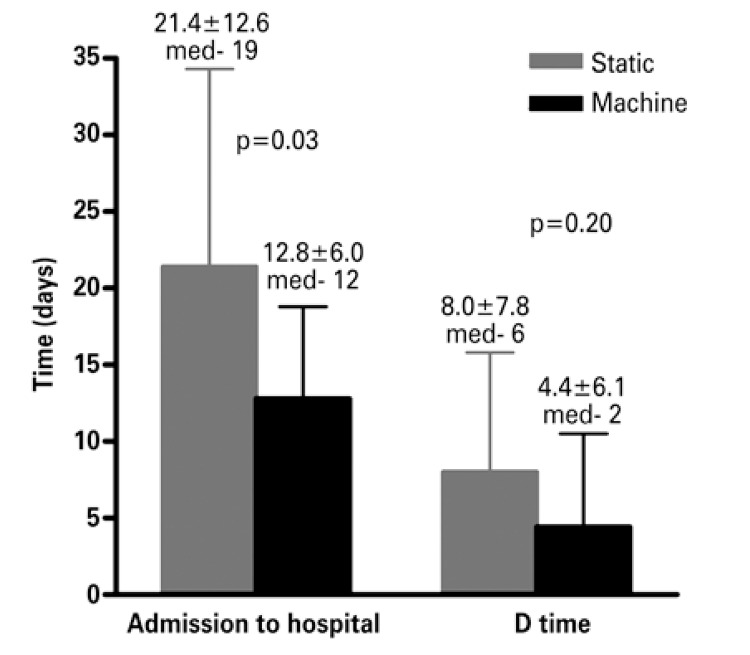
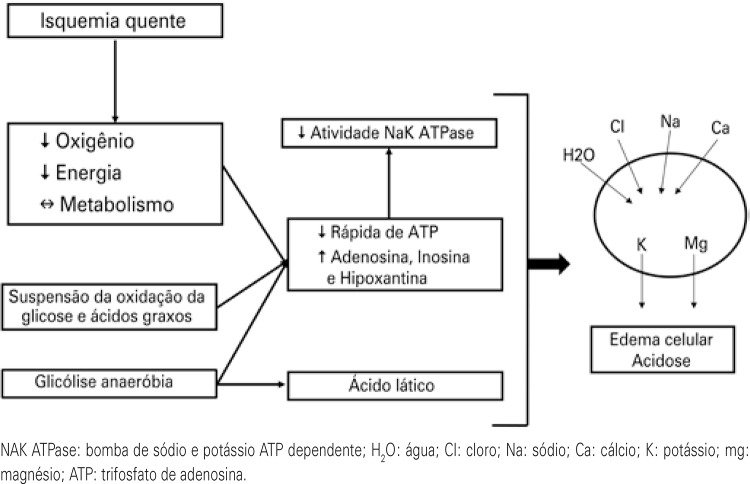
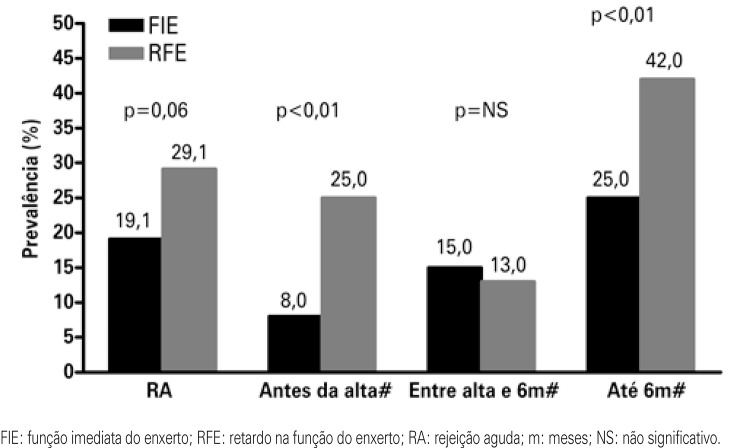
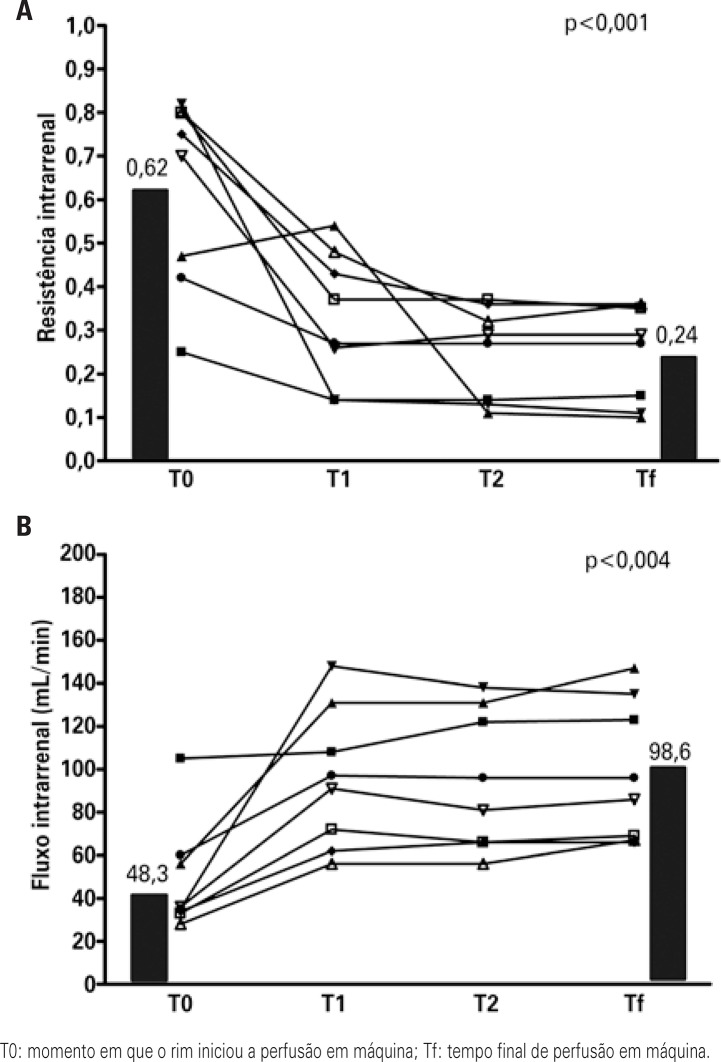
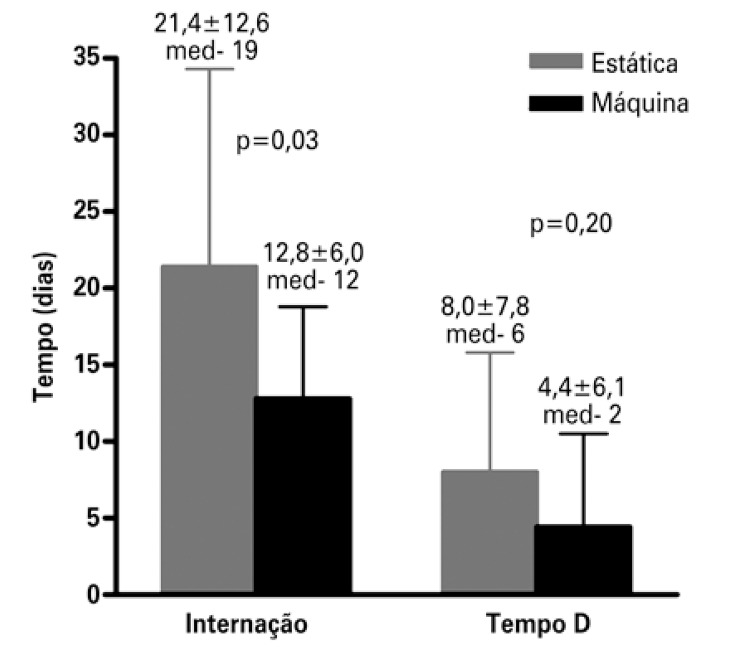
Ischemia and reperfusion injury is an inevitable event in renal transplantation. The most important consequences are delayed graft function, longer length of stay, higher hospital costs, high risk of acute rejection, and negative impact of long-term follow-up. Currently, many factors are involved in their pathophysiology and could be classified into two different paradigms for education purposes: hemodynamic and immune. The hemodynamic paradigm is described as the reduction of oxygen delivery due to blood flow interruption, involving many hormone systems, and oxygen-free radicals produced after reperfusion. The immune paradigm has been recently described and involves immune system cells, especially T cells, with a central role in this injury. According to these concepts, new strategies to prevent ischemia and reperfusion injury have been studied, particularly the more physiological forms of storing the kidney, such as the pump machine and the use of antilymphocyte antibody therapy before reperfusion. Pump machine perfusion reduces delayed graft function prevalence and length of stay at hospital, and increases long-term graft survival. The use of antilymphocyte antibody therapy before reperfusion, such as Thymoglobulin™, can reduce the prevalence of delayed graft function and chronic graft dysfunction.
A lesão de isquemia e reperfusão é um evento inevitável no transplante de rim, tendo como consequências retardo na função do enxerto, aumento no tempo de hospitalização e dos custos, aumento no risco de rejeição aguda e potencial impacto negativo na evolução a longo prazo. Atualmente, vários fatores estão implicados na fisiopatologia da lesão de isquemia e reperfusão, podendo ser didaticamente divididos em dois paradigmas: hemodinâmico e imunológico. O paradigma hemodinâmico é classicamente descrito como a privação de oxigênio pela interrupção do fluxo sanguíneo, envolvendo diversos sistemas hormonais e pela produção de radicais livres de oxigênio após a reperfusão. O paradigma imunológico tem sido descrito mais recentemente e envolve as células do sistema imune, sobretudo as células T, como papel fundamental na lesão. De acordo com esses conceitos, novas estratégias de prevenção dos impactos da lesão de isquemia e reperfusão têm sido estudadas, especialmente formas mais fisiológicas de preservação do órgão, como a preservação em máquina de perfusão e o uso de anticorpos depletores de linfócitos antes da reperfusão. A perfusão em máquina reduz a prevalência de retardo na função do enxerto e o tempo de hospitalização, além de melhorar a sobrevida do enxerto a longo prazo. Já o uso de anticorpos depletores de linfócitos, como Timoglobulina®, antes da reperfusão, pode diminuir a prevalência de retardo na função do enxerto e a disfunção crônica do mesmo.
Figures
References
-
- Molitoris BA. Ischemic acute renal failure: exciting times at our fingertips. Curr Opin Nephrol Hypertens. 1998;7(4):405–406. - PubMed
-
- Waikar SS, Liu KD, Chertow GM. Diagnosis, epidemiology and outcomes of acute kidney injury. Clin J Am Soc Nephrol. 2008;3(3):844–861. - PubMed
-
- Brady H, Singer GG. Acute renal failure. Lancet. 1995;346(8989):1533–1540. Review. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
