

Magnetic resonance enterographic predictors of one-year outcome in ileal and ileocolonic Crohn's disease treated with anti-tumor necrosis factor antibodies
- PMID: 25993615
- PMCID: PMC4438711
- DOI: 10.1038/srep10223
Magnetic resonance enterographic predictors of one-year outcome in ileal and ileocolonic Crohn's disease treated with anti-tumor necrosis factor antibodies
Abstract
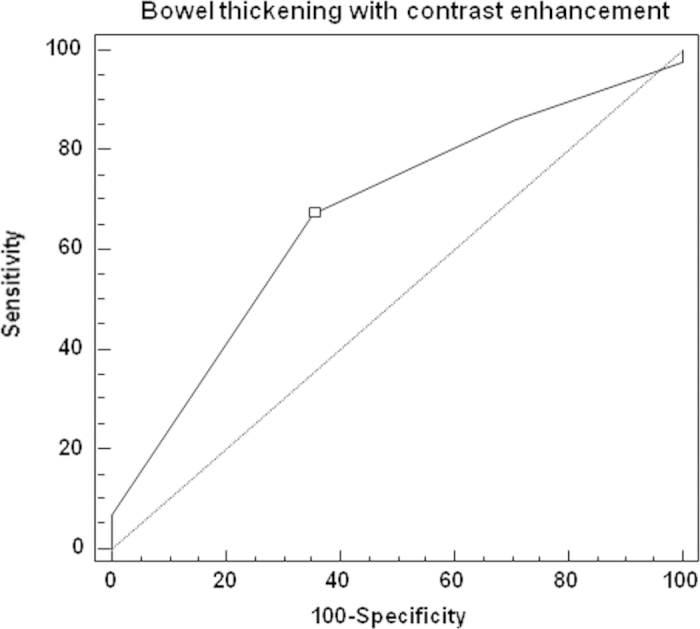
The aim of the study was to assess the role of magnetic resonance enterography (MRE) in predicting one-year efficacy of anti-tumor necrosis factor antibodies--infliximab (IFX), adalimumab (ADA) in Crohn's disease (CD) patients primarily responding to therapy. We performed retrospective analysis among 61 CD patients who had undergone a successful IFX/ADA induction therapy and were treated with maintenance doses. All patients underwent MRE at week 0. We assessed which MRE features were predictive for steroid-free remission at week 52, and which were associated with a secondary loss of response. 44 patients were in steroid-free remission at week 52, 17--were secondary non-responders. The ROC curve showed that bowel thickening with contrast enhancement analyzed together at week 0 were associated with steroid-free remission at week 52 (p = 0.01; AUC 0.67). Bowel stenosis with or without prestenotic dilatation [OR 5.8 (95% CI 1.4-25) and 2.4 (95% CI 1.2 - 5) respectively; p = 0.01] and the presence of intra-abdominal fistulas [OR 1.4 (95% CI 1.1-2); p=0.004] were related to secondary non-response. A high baseline inflammatory activity detected by MRE predicts one-year response in CD after IFX/ADA. In case of bowel stenosis, intra-abdominal fistulas, other therapeutic options should be considered.
Conflict of interest statement
PE, LLS, and KK received lecture fees from Abbvie Poland. Other authors declare no competing financial interests.
Figures
References
-
- Feagan B. G. et al. Recommendations for the treatment of Crohn’s disease with tumor necrosis factor antagonists: an expert consensus report. Inflamm. Bowel Dis. 1, 152–160 (2012). - PubMed
-
- Allez M. et al. Report of the ECCO pathogenesis workshop on anti-TNF therapy failures in inflammatory bowel diseases: definitions, frequency and pharmacological aspects. J. Crohns Colitis 4, 355–366 (2010). - PubMed
-
- Amitai M., Ben-Horin S., Eliakim R. & Kopylow U. Magnetic resonance enterography in Crohn’s disease: a guide to common imaging manifestations for the IBD physician. J. Crohns Colitis 8, 603–615 (2013). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
